
🌩️ Taming the Storm: Managing the Violent & Aggressive Child in the Emergency Department
A practical guide for the ED clinician or paediatrician


You’re halfway through a packed night shift. A 9-year-old with a history of oppositional defiant disorder arrives by ambulance with police escort. He’s biting, spitting, throwing things. Staff are scared. Parents are crying. The waiting room is watching.
What do you do?
Before we begin: the best restraint is the one you never need to use.
📈 The Elephant in the Resus Bay: This Problem is Getting Bigger
Paediatric mental and behavioural health (MBH) visits to the emergency department have more than doubled between 2009 and 2019. Up to 12% of children seen in the ED for mental health complaints receive intramuscular medication for acute agitation, and 5 to 10% are physically restrained.
In 2021, the American Academy of Pediatrics (AAP), the American Academy of Child and Adolescent Psychiatry (AACAP) and the Children’s Hospital Association jointly declared a national emergency in child and adolescent mental health.
😮 Over 79 paediatric deaths have been attributed to restraint-related events in the United States alone.
This is not a niche topic. And we need to get it right.
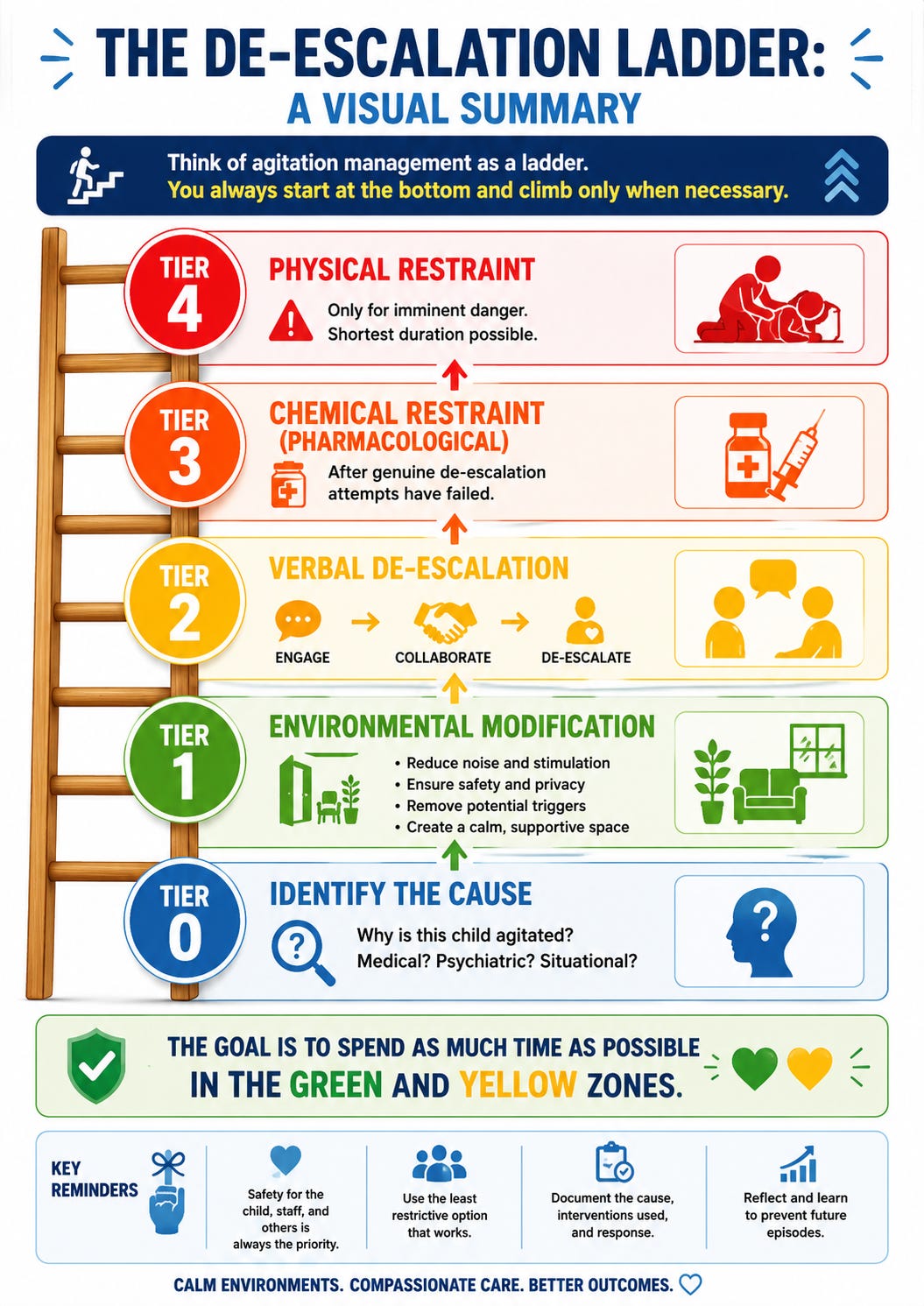
🧩 Tier 0: Understand WHY the Child Is Agitated
Before reaching for midazolam, take a breath. 🫁
The AAEP (American Association for Emergency Psychiatry) BETA Consensus Statement is crystal clear: agitation is a symptom, not a diagnosis. Just like pain points to a source, agitation points to an underlying driver.
Common aetiologies in children include:
🧠 Psychiatric: Psychosis, mania, severe anxiety, PTSD, oppositional defiant disorder (ODD), conduct disorder
🧪 Toxic: Substance intoxication or withdrawal (yes, even in kids)
🤕 Medical/Organic: Hypoglycaemia, head injury, sepsis, hypoxia, pain, urinary retention
♿ Neurodevelopmental: Autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), intellectual disability with sensory overwhelm
💔 Situational: Fear, loss of control, unfamiliar environment, separation from carers
📌 Clinical Pearl: Neurodivergent children (especially those with ASD or ADHD) may communicate distress differently. A thorough history and physical examination is essential before attributing the behaviour to a purely psychiatric cause.
🟢 Tier 1: Environmental Modification (Your First Move)
Before anyone says a single word, change the environment. The ED itself can be a massive agitation trigger.
What the Evidence Says 📚
The 2024 ACEP Pediatric Emergency Medicine Committee review by Saidinejad et al. specifically highlights how the ED environment worsens agitation:
💡 Intense, harsh lighting
📢 Loud, chaotic noise
🌡️ Poorly regulated temperature
🚫 Lack of familiar objects
👥 Crowding and constant interruptions from staff
🍽️ No access to food or drink
😣 Physical discomfort (restraints, IV lines, monitors)
Your Environmental Checklist ✅

📌 Clinical Pearl: For children boarding overnight in the ED awaiting psychiatric placement, using a quieter area of the ED (such as an urgent care zone that closes at night) can help preserve circadian rhythms and reduce overnight escalation events.
🟡 TIER 2: Verbal De-escalation (Your Most Powerful Tool) 🗣️
This is the cornerstone of agitation management. The AAEP Project BETA De-escalation Workgroup describes a 3-step approach:
The 3-Step Framework
Step 1: Engage 🤝
Approach calmly, at eye level
Introduce yourself
Use a soft, slow, low-pitched voice
Maintain a non-threatening posture (hands visible, no crossed arms)
Respect personal space (at least one arm’s length)
Step 2: Collaborate 🧩
Ask what’s bothering them
Listen actively without interrupting
Validate their feelings (”I can see you’re really upset”)
Offer choices (”Would you like to sit on the bed or in the chair?”)
Include the child in decision-making
Step 3: De-escalate 🌊
Set clear, simple limits (”I need you to stop throwing things so we can help you”)
Offer concrete alternatives (”You can squeeze this stress ball instead”)
Negotiate achievable goals (”If you can sit down for 5 minutes, I’ll get you that juice”)
Praise any positive behaviour immediately
What Does This Look Like in Real Life? 🎬
Imagine a 12-year-old girl with known PTSD, brought in after a self-harm episode, now screaming and pulling at her IV line.
❌ Wrong approach: “Stop that! You need to calm down! Security!”
✅ Right approach: Kneel to her level. Soft voice. “Hey. I’m Dr. K. I can see this is really scary for you. Can you tell me what’s making things worse right now? ... The IV is hurting? OK. Let me see if we can take a break from that. Would you like some water while we figure this out together?”
📌 Clinical Pearl: A case report by Croce and Mantovani (2017) demonstrated how a consistent, dedicated provider using verbal and behavioural de-escalation prevented the need for physical restraint in a child who had been restrained multiple times in prior ED visits.
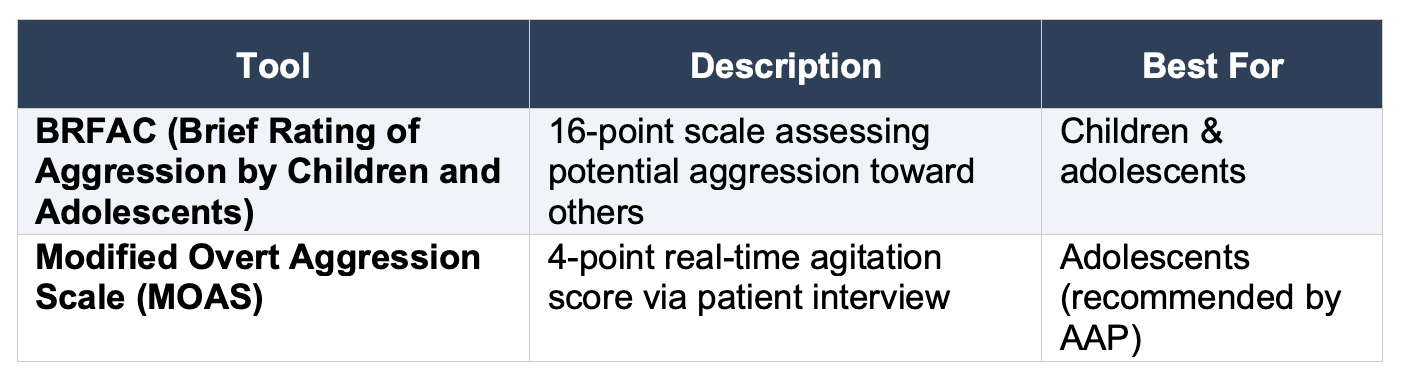
⚠️ TIER 2.5: Agitation Scoring and Team Readiness
Before escalation spirals, quantify the risk and rally your team.
Personalised De-escalation Plans 📋
One of the most impactful quality improvement strategies from Hoffmann et al. (2023) was the introduction of personalised de-escalation plans for high-risk patients. These plans document:
Known triggers (noise? touch? specific people?)
Successful calming strategies from prior visits
Preferred medications and routes
Parent/carer input
This information should be recorded, communicated during handovers, and updated with each visit.
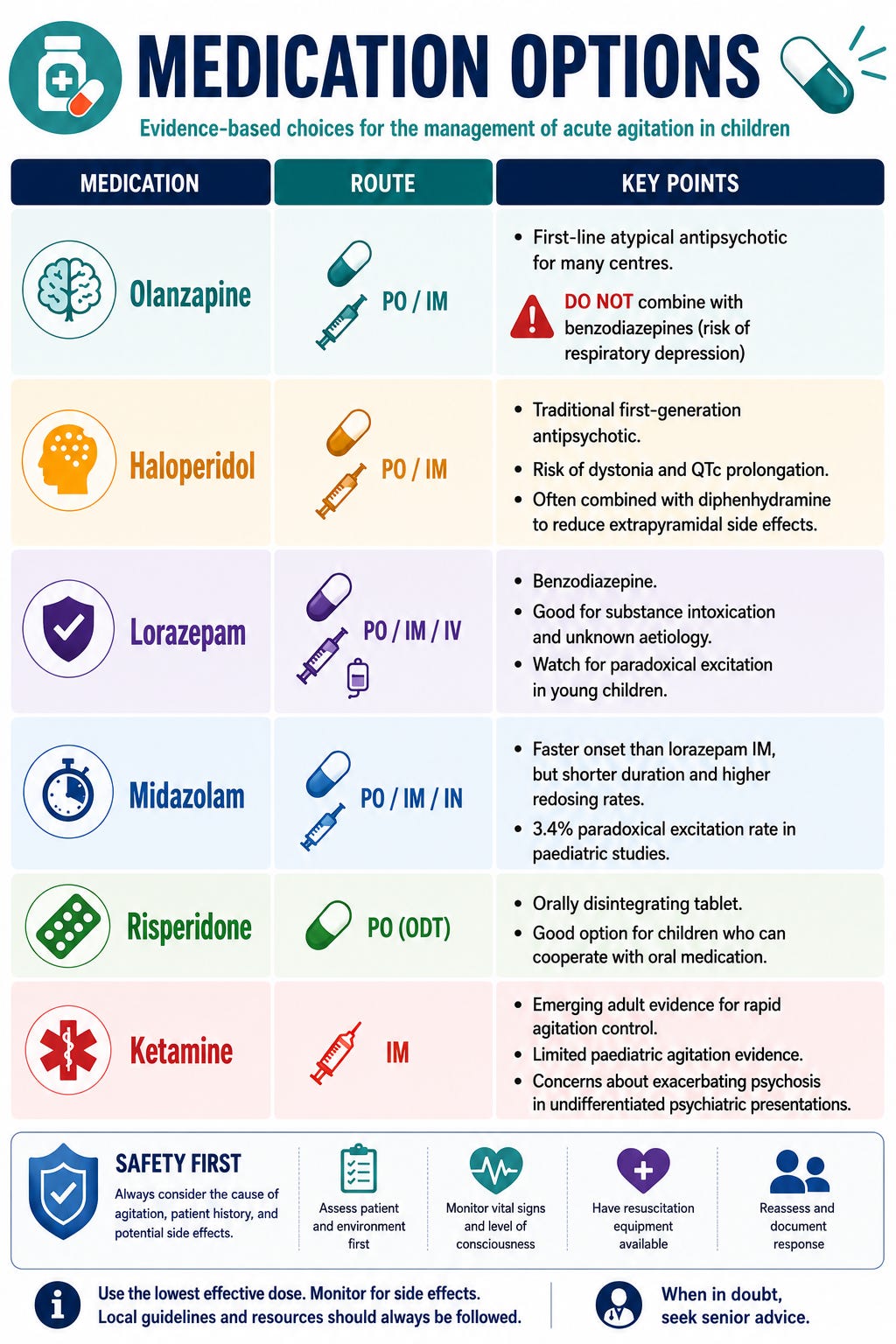
🔴 TIER 3: Chemical Restraint (When All Else Has Failed)
Let’s be absolutely clear. 🛑
Chemical (pharmacological) restraint should only be considered after environmental modification and verbal de-escalation have been genuinely attempted and have failed. This is not optional. This is the standard of care.
The AAEP BETA Consensus Principles:
Agitation management should be individualised, multidisciplinary and collaborative
The aetiology of agitation should drive the choice of treatment
Medication should be ONE part of a comprehensive strategy
Consider an extra dose of a home medication first (it’s familiar, better tolerated, fewer drug interactions)
Avoid over-sedation (a child who cannot participate in their own assessment cannot be properly evaluated)
🔴🔴 TIER 4: Physical Restraint (The Absolute Last Resort)
Physical restraint in a child is traumatic. For the child. For the parents. For the staff. And it can be lethal.
Key Principles from the Evidence 📚
Physical restraint should be used only when there is imminent danger of harm to the patient or others, and all other strategies have been exhausted
It should be applied using the least restrictive means for the shortest possible duration
The patient must be continuously monitored during restraint (vital signs, airway, circulation to extremities, emotional state)
Restraint is never therapeutic. It is a safety intervention only
Disparities Matter ⚖️
This is important and often overlooked. Evidence shows disparities in restraint use across racial and ethnic lines. Black and brown youth are more likely to be physically restrained compared to white youth, even after controlling for acuity. Training in trauma-informed, culturally responsive care and the use of standardised agitation pathways can help reduce these disparities.
Training Gaps Are Real 🎓
A study by Dorfman and Kastner (2004) found that a large percentage of emergency medicine and paediatric emergency medicine residency programmes do not teach trainees about the appropriate application of restraints or the clinical situations warranting their use. This has to change.
👨👩👧 Talking to Parents: The Conversation That Matters Most
This is the part many clinicians dread. But done well, it transforms the encounter.
Before Escalation 🕐
Introduce yourself and your role clearly
Explain the situation in plain language: “Your child is very distressed right now and is at risk of hurting themselves or others. We are going to try everything we can to help them calm down safely.”
Involve parents as partners: Ask about triggers, calming strategies, medications
Set expectations: “If the de-escalation strategies don’t work, we may need to use medication to help them feel calmer and safer. I will keep you informed every step of the way.”
During Restraint (Physical or Chemical) 💬
Narrate what is happening and why: “We’re giving your child a medication that will help them relax. This is to keep them safe.”
Validate their distress: “I know this is incredibly hard to watch. You’re not failing your child. This is a medical situation and we are here to help.”
Offer presence or privacy: Some parents want to stay; some need to step out. Both are OK. Ask them.
Designate a team member to stay with the family and answer questions in real time
After the Event 🌅
Debrief with the family: Explain what happened, what medications were given, and what the plan is going forward
Screen for caregiver distress: Parents who witness their child being restrained can develop secondary traumatic stress
Document the de-escalation plan for future visits
Connect with outpatient resources: Mental health follow-up, crisis plans, school-based supports
🧠 Key Takeaways for the Busy ED Clinician
🔍 Always look for a treatable cause before labelling behaviour as “psychiatric”
🏠 Modify the environment first: Dim lights, reduce noise, offer comfort items and food
🗣️ Invest in verbal de-escalation: This is your most powerful and safest tool
📊 Use agitation scores and personalised de-escalation plans to standardise care
💊 When medication is needed, choose based on aetiology: Prioritise home medications, use the least sedating effective option, and never combine olanzapine with benzodiazepines
🛑 Physical restraint is the absolute last resort: Monitor continuously, use the least restrictive means, and aim for the shortest duration
👨👩👧 Communicate with parents proactively, honestly and compassionately: They are partners in care, not bystanders
📝 Document everything: Triggers, strategies tried, medications given, and plans for future visits
⚖️ Be aware of disparities: Standardised pathways help ensure equitable care
💪 Debrief your team: This work is emotionally taxing. Staff wellbeing matters too
Enjoyed this post? 🙌 Share it with your ED team. Bookmark it for your next shift.
And remember: the best restraint is the one you never need to use.Stay safe out there. 💛🩺