
Paediatric Sepsis 2026: The Surviving Sepsis Campaign Guidelines Are Here
The most comprehensive update to paediatric sepsis care in six years dropped on March 23, 2026. Is it practice changing?

Sepsis remains one of the most time-critical, brain-eating diagnoses you will face in the paediatric emergency department. The 2026 Surviving Sepsis Campaign (SSC) guidelines are a full rebuild from the 2020 version, with hard answers to questions that have haunted resuscitation bays for years. Let’s go.
At a glance:
61 total statements
5 strong recommendations
24 conditional recommendations
10 good practice statements
20 brand-new topics covered for the first time
🧩 1. What Even IS Paediatric Sepsis Now? Hello, Phoenix.

The old SIRS-based definition is retired. The 2024 Phoenix Sepsis Definitions Taskforce gave us a data-driven, organ-dysfunction-centred framework and the 2026 SSC guidelines are built on it.
📌 Phoenix Sepsis Definition (2024)
Sepsis = Suspected infection + Phoenix Sepsis Score ≥ 2 points, indicating life-threatening organ dysfunction in the respiratory, cardiovascular, coagulation or neurological systems
Septic Shock = Sepsis + ≥ 1 cardiovascular dysfunction point: severe age-appropriate hypotension, venous or arterial lactate > 5 mmol/L, or need for vasoactive medication
The Phoenix score covers 4 organ systems:
🫁 Respiratory — SpO2/FiO2 ratio, ventilator support (0–3 points)
❤️ Cardiovascular — blood pressure, lactate, vasoactive medications (0–6 points)
🩸 Coagulation — platelets, INR, D-dimer, fibrinogen (0–2 points)
🧠 Neurological — GCS, pupillary response (0–2 points)
Threshold: Phoenix score ≥ 2 = Sepsis
The score ≥ 2 threshold identifies children at the highest risk of mortality — irrespective of SIRS criteria, which have notoriously poor specificity. SIRS is dead. Know Phoenix.
🔍 2. Recognition and Screening — The Uncomfortable Truth
⚠️ Insufficient evidence:
There was insufficient evidence to recommend implementing systematic sepsis screening tools (in addition to established clinical protocols) for the timely recognition of sepsis and septic shock in acutely unwell children.
Don’t misread this. The panel is NOT saying screening is bad. They are saying that adding a screening tool on top of solid clinical protocols hasn’t been proven to add value. Your clinical protocols for triage and identification of the sick child? Keep them sharp. This is NOT permission to be passive.
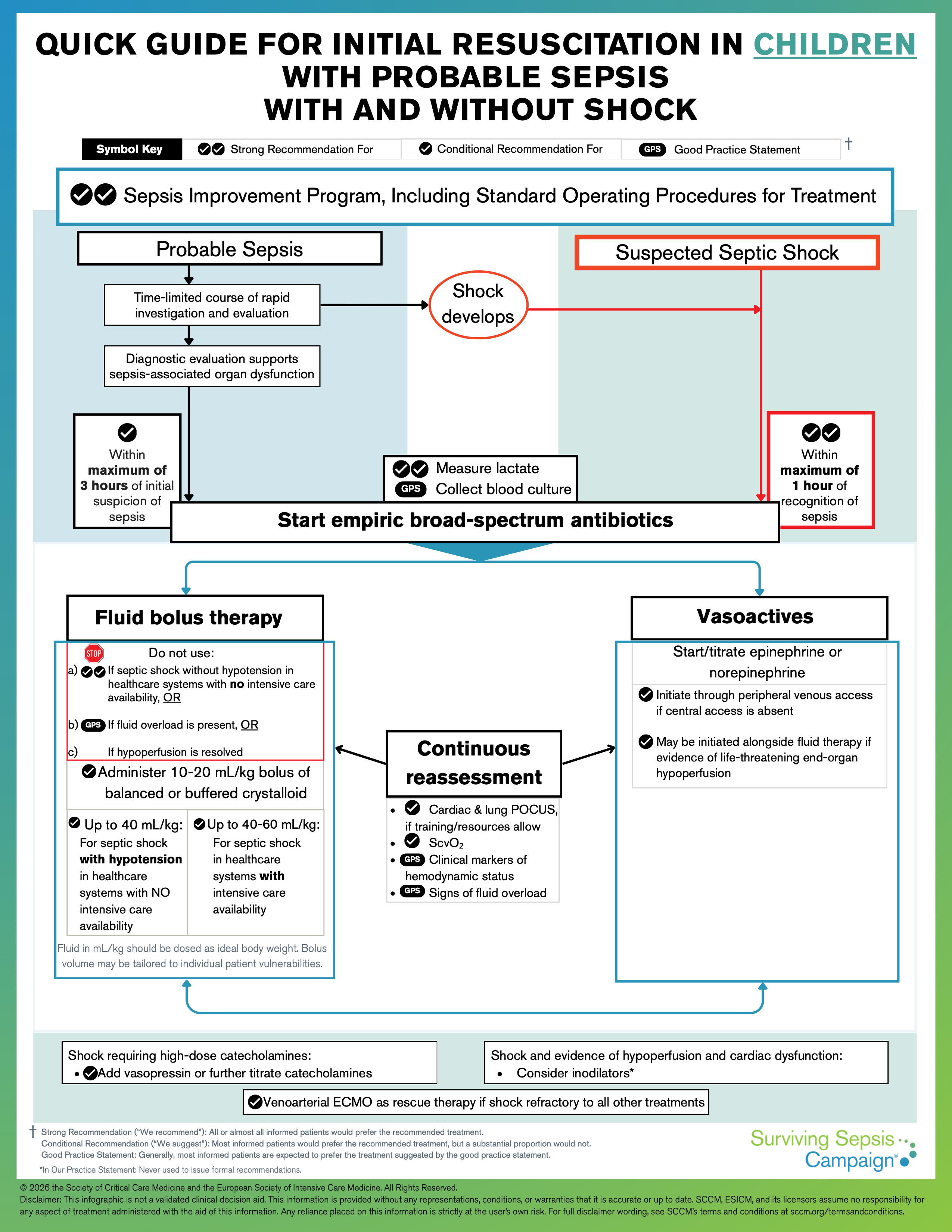
💪 STRONG recommendation: Hospitals must implement a performance improvement program with standard operating procedures for the treatment of children with sepsis or septic shock. (Certainty: Low — but this is non-negotiable operationally.)
⚡ ED Bottom Line: No validated screening tool to mandate, but your department must have a written sepsis protocol. If you don’t have one, this guideline is the push to build it.
🧪 3. Diagnostics — What to Measure Before You Treat
Blood Cultures
✅ Good Practice Statement: Obtain blood cultures before initiating antimicrobial therapy — provided this does not substantially delay treatment. Unchanged from 2020.
The key word is “substantially.” Do not delay antibiotics chasing a blood culture.
Lactate
💪 Recommended: Measure blood lactate as part of the initial evaluation and management of children with probable sepsis or suspected septic shock. (Certainty: Very low — but clinically essential.)
Lactate ≥ 5 mmol/L now defines cardiovascular dysfunction in the Phoenix score. This is not just a resuscitation endpoint. It is part of your diagnostic criteria.
Molecular / Rapid Pathogen Testing
⚠️ Insufficient evidence — NEW: No recommendation for or against routine molecular testing for pathogen detection in children with probable sepsis or suspected/confirmed septic shock.
The technology is exciting.
The outcome evidence is not there yet.
💧 4. Fluid Resuscitation — Context Is Everything
This is where the 2026 guidelines earn their keep. Fluid resuscitation is now explicitly stratified by healthcare system capacity.
Setting: ICU Available + Septic Shock
🔵 Conditional: Administer up to 40–60 mL/kg total fluid, in 10–20 mL/kg boluses, over the first hour of initial resuscitation. (Certainty: Low)
Setting: No ICU Available + Sepsis WITHOUT Hypotension
🚫 STRONG recommendation AGAINST fluid bolus: Start maintenance fluids only. (Certainty: HIGH)
This is one of the highest-certainty statements in the entire document. Fluid boluses in sepsis without hypotension in resource-limited settings cause harm.
Full stop.
Setting: No ICU Available + Septic Shock WITH Hypotension
🔵 Conditional: Administer up to 40 mL/kg total in 10–20 mL/kg boluses over the first hour. (Certainty: Low)
🚨 NON-NEGOTIABLE: Reassess after EVERY bolus.
Stop if shock resolves OR if any signs of fluid overload appear. Signs that should stop your boluses include clinical pulmonary oedema and new or worsening hepatomegaly. Reassess using: heart rate, blood pressure, capillary refill time, level of consciousness, urine output.
What fluid to use?
🔵 Conditional: Crystalloids over albumin for initial resuscitation. (Certainty: Moderate)
🔵 Conditional: Balanced or buffered crystalloids (Hartmann’s solution, lactated Ringer’s) over 0.9% saline. (Certainty: Very low)
If balanced crystalloids are not available, 0.9% saline is an acceptable alternative.
💊 5. Antimicrobials — Time Is Tissue
The timing recommendations are clearer than ever. The 2026 SSC draws a sharp line between septic shock and probable sepsis without shock.
💪 STRONG recommendation: For children with suspected septic shock — start antimicrobials as soon as possible, ideally within 1 hour of recognition. (Certainty: Very low — clinical urgency drives this, not just RCT data.)
🔵 Conditional: For probable sepsis without shock — allow a time-limited rapid investigation period. If concern is substantiated, start antimicrobials ideally within 3 hours of recognition. (Certainty: Very low)
✅ Good Practice Statement: Empiric broad-spectrum therapy covering all likely pathogens. If immunocompromised or high MDR (multidrug-resistant organism) risk: use empiric multi-drug therapy.
⚡ The Clock Rule:
Shock = antibiotics within 1 hour ⏱️
Sepsis without shock = antibiotics within 3 hours ⏱️⏱️⏱️
Blood cultures first — but NEVER delay antibiotics to get them.
💉 6. Vasoactive Medications — Do Not Wait for a Central Line
🔵 Conditional — NEW 2026: For children with septic shock requiring vasoactive medications, initiate via peripheral venous access rather than delaying until central venous access is obtained. (Certainty: Very low)
⚠️ Insufficient evidence: No recommendation on whether epinephrine or norepinephrine is preferred as first-line vasopressor in children with septic shock.
⚠️ Insufficient evidence: No recommendation on whether to start vasoactives before or after 40 mL/kg of bolus fluid therapy in septic shock.
⚡ What this means in practice:
Don’t hold off on vasopressors waiting for a PICC or CVC. Get peripheral IV access working. Noradrenaline and adrenaline are both defensible first-line choices - let local protocol and clinical experience guide you.
🔊 7. POCUS — The New Kid in the Guidelines
🔵 Conditional — NEW 2026: For children with sepsis or septic shock, use cardiac and lung point-of-care ultrasound (POCUS) to guide resuscitation over not using POCUS — IF local training and resources allow. (Certainty: Low)
[🖼️ IMAGE EMBED: POCUS cardiac views in paediatric emergency] Search: “paediatric POCUS sepsis cardiac views” — RadioGraphics and ACEP have excellent free images
This is a big deal. POCUS lets you see IVC collapsibility, cardiac contractility and lung pathology in real time — titrating fluids and vasopressors with eyes instead of guesswork. The guidelines acknowledge the research gap and call for more outcome data, but they want you to use it if you have the skill.
The conditional language matters — this is not a mandate. It is an endorsement of capability.
🌬️ 8. Oxygen Targets — Conservative Is the New Gold
🔵 Conditional — NEW 2026: For children with sepsis or septic shock following resuscitation, titrate supplemental oxygen to a conservative SpO2 target of 88–92%, NOT a liberal target of > 94%. (Certainty: Moderate — one of the strongest evidence grades in the 2026 document.)
💚 Why conservative oxygen?
Hyperoxia causes pulmonary vasoconstriction, oxidative stress and free radical damage. In a post-resuscitation child, targeting SpO2 88–92% reduces oxygen toxicity without evidence of harm. This shifts standard practice significantly from the “100% O2 always good” era.
This applies after resuscitation — not during active shock management.
❌ 9. Etomidate — Still on the Banned List
🔵 Conditional — against use: For children with sepsis or septic shock requiring intubation, do NOT use etomidate. (Certainty: Low)
Etomidate suppresses cortisol synthesis via adrenal inhibition, potentially worsening the adrenal crisis component of sepsis. Ketamine remains your RSI agent of choice for the haemodynamically compromised child. Etomidate was already out in most paediatric guidelines — 2026 doubles down.
💊 10. Corticosteroids — Nuanced, Not Blanket
🔵 Conditional — against: For children with septic shock where haemodynamic stability can be restored with fluid resuscitation and vasoactive therapy: do NOT use IV hydrocortisone. (Certainty: Low)
⚠️ Insufficient evidence: For children with fluid-refractory, catecholamine-resistant septic shock: no recommendation for or against IV hydrocortisone.
✅ Good Practice Statement: Stress-dose corticosteroids must be administered for suspected or documented adrenal insufficiency. Routine steroids are not recommended — but adrenal insufficiency changes everything.
⚡ Bottom line on steroids:
Responds to fluids and vasopressors → no steroids.
Catecholamine-resistant + suspected adrenal insufficiency → give stress-dose steroids.
Refractory shock without clear adrenal insufficiency → clinical judgment, no firm guidance.
🧠 11. Other Metabolic and Adjunctive Therapy
⚠️ Insufficient evidence: No recommendation on sodium bicarbonate for metabolic acidaemia in sepsis.
🔵 Conditional — against: Do not use routine levothyroxine in children with septic shock in a sick euthyroid state. (Certainty: Low)
⚠️ Insufficient evidence: No recommendation on targeting normal calcium levels versus tolerating hypocalcaemia.
⚠️ Insufficient evidence: No recommendation on targeting normothermia versus permissive fever.
🏥 12. Post-Sepsis: The Chapter the 2020 Guidelines Never Had
This is a landmark addition to the 2026 guidelines. For the first time, the SSC paediatric guidelines explicitly address post-sepsis morbidity and long-term follow-up. This is not just an ICU problem. It is an ED problem, a family problem and a health system problem.
📌 Among children who survive ICU-level sepsis treatment, 30–40% will face lasting health consequences. We are discharging children who look better but may not be better.
Post-sepsis sequelae to recognise:
🧠 Neurocognitive impairment — executive dysfunction, learning difficulties
😰 Psychological sequelae — PTSD in children AND caregivers
💪 Physical deconditioning and functional limitation
❤️ Organ-specific complications: cardiac, pulmonary, renal
💚 Clinical Implication
Children discharged after a sepsis admission need a structured follow-up plan. This is increasingly the ED’s job to initiate — the referral letter, the warning to the paediatrician, the conversation with the family. The 2026 guidelines put this on the map for the first time.
🚫 The “Don’t Do” List — Quick Reference Table
RecommendationStrength
❌ Fluid bolus in sepsis WITHOUT hypotension (no ICU available)
❌ Etomidate for intubation in sepsis (Conditional against)
❌ Hydrocortisone if haemodynamically stable on fluids + vasopressors (Conditional against)
❌ Levothyroxine in sick euthyroid state (Conditional against)
❌ Liberal SpO2 targets (>94%) post-resuscitation(Conditional against)
❌ Delaying vasopressors until central line obtained (Conditional against)
❌ Albumin over crystalloids for initial resuscitation (Conditional against)
⚡ The Spoon Fed Takeaway
Phoenix ≥ 2 = sepsis. Lactate ≥ 5 + cardiovascular dysfunction = septic shock.
Shock → antibiotics within 1 hour. Sepsis without shock → antibiotics within 3 hours.
Fluids: 10–20 mL/kg boluses, reassess after each, stop at signs of overload.
No ICU + no hypotension = NO boluses. Strong recommendation. High certainty.
Vasopressors via peripheral IV. Do not wait for a central line.
SpO2 88–92% after resuscitation. Conservative oxygen is the new standard.
Avoid etomidate. Think about post-sepsis follow-up before every discharge.
📚 Key References and Resources
Full guideline (Intensive Care Medicine):
Published in Pediatric Critical Care Medicine and Intensive Care Medicine | Endorsed by 14 organisations | Weiss S et al. Pediatr Crit Care Med. 2026 Mar 23. doi: 10.1097/PCC.0000000000003927 - https://doi.org/10.1007/s00134-026-08360-2SCCM interactive recommendation filter: https://www.sccm.org/clinical-resources/guidelines/guidelines/surviving-sepsis-campaign-international-guidelines-for-the-management-of-sepsis-and-septic-shock-in
Official paediatric quick guide infographic (free PDF):https://mcusercontent.com/acff250cf3d0418bbe904af42/files/640adb17-9ef2-6c34-398e-b5a43624a87b/SSC_Children_Quick_Guide_Infographic_2026.01.pdf
Phoenix Sepsis Criteria — open access review: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11239205/
ESICM 2026 SSC launch page (all infographics, adult and paediatric): https://www.esicm.org/2026-surviving-sepsis-campaing-guidelines/
PubMed citation: https://pubmed.ncbi.nlm.nih.gov/41870559/