
🫁 Tiny Lungs, Huge Stakes: The 4 Physiological Truths That Will Change How You Ventilate Kids
Spoon Fed PEM | Paediatric Ventilation Series | Part 1


Everything about managing a child’s airway and lungs is different.
Not slightly different. Fundamentally different.
The margins are thinner. The physiology is less forgiving. And the anatomy is working against you in ways that adult practice never prepares you for. 😤
This Spoon Fed PEM covers the four things that matter most at the bedside:
🔺 Airway geometry 🦴 Chest wall compliance 🔥 Oxygen consumption 💨 Functional residual capacity
Get these wrong and you are behind before you have even touched the ventilator.
Let’s break them down. ⬇️
1️⃣ The Airway Is a Funnel, Not a Cylinder 🔺
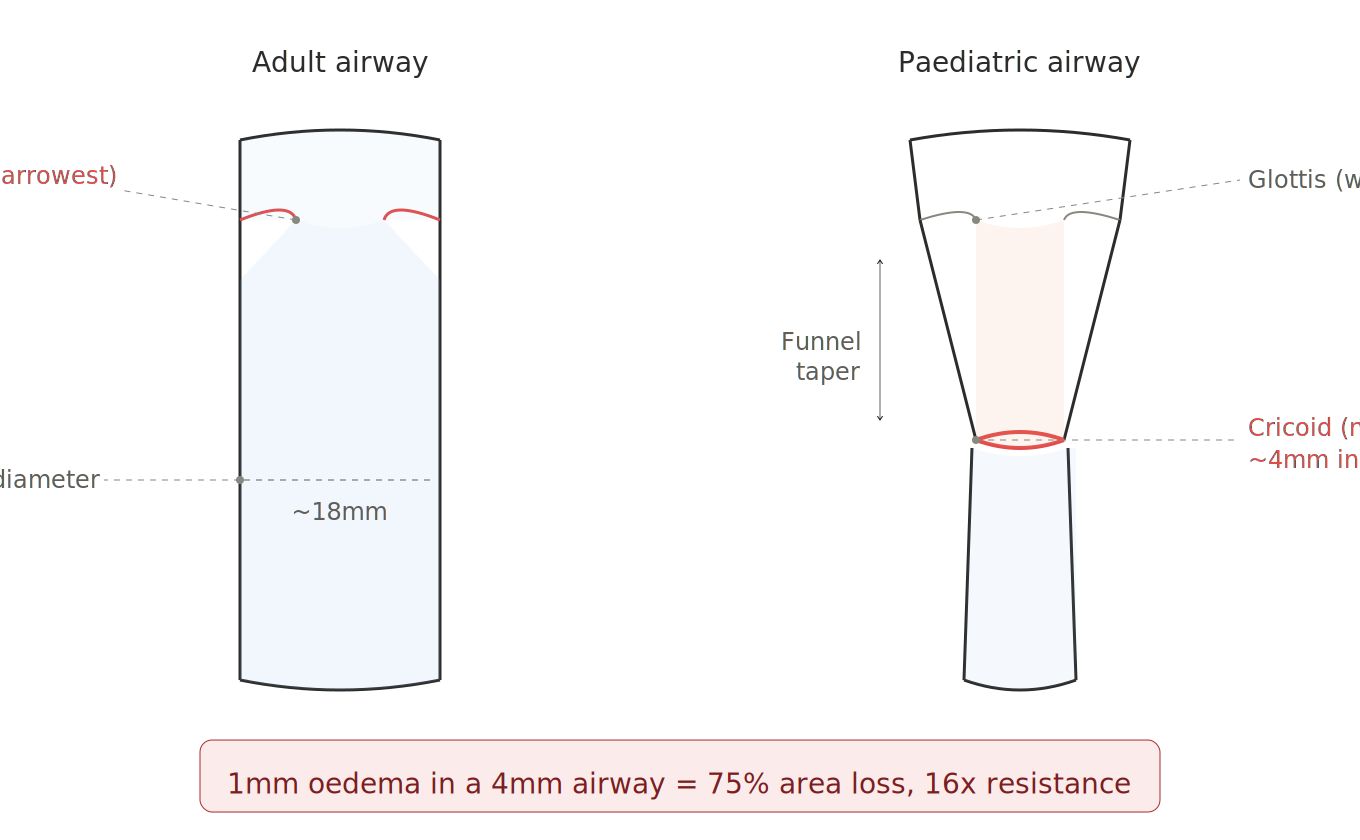
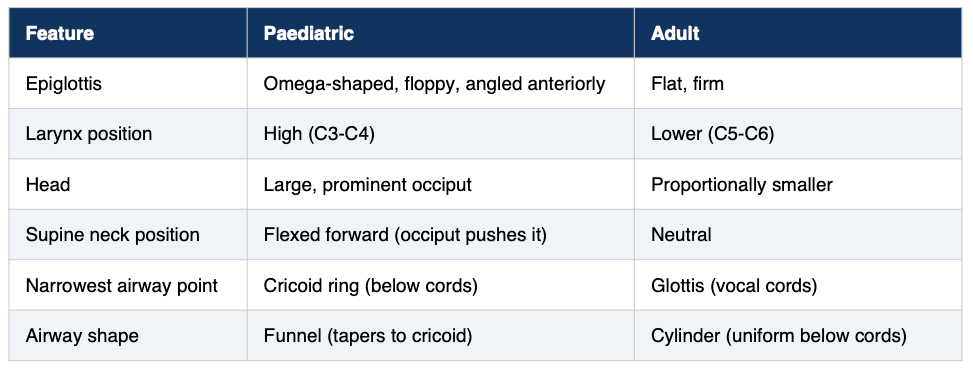
In adults, the narrowest point of the airway is the glottis (the vocal cords). Below the cords, the trachea is a roughly uniform cylinder. Simple enough.
In children under ~8 years old, the game changes completely.
The narrowest point is the cricoid ring, sitting below the cords. The airway tapers from the laryngeal inlet down to the cricoid like a funnel. 🫠
Why does this matter?
Two big reasons:
🔸 Reason 1: An ETT that passes the cords easily can still jam at the cricoid or create a pressure point there. The cords are not the final checkpoint in kids.
🔸 Reason 2: Even 1mm of mucosal oedema has a catastrophic effect on resistance.
🧮 The Maths That Should Scare You
In a 4mm infant airway, 1mm of circumferential swelling reduces the cross-sectional area by roughly 75% and increases resistance by a factor of 16.
That is Poiseuille’s law in action:
Resistance ∝ 1/r⁴
Resistance is inversely proportional to the fourth power of the radius.
A 1mm reduction is nothing in an adult. It is everything in an infant. 😳
🧠 Don’t Forget the Other Anatomical Curveballs
🎯 Clinical Pearl
You have almost no room for error with tube sizing in small children. Any condition causing airway swelling (croup, post-extubation oedema, burns) can become life-threatening fast. A half-size-too-large tube creates subglottic injury. A half-size-too-small tube creates an unacceptable leak. Size matters. A lot. 🫣
2️⃣ The Chest Wall Is Too Compliant 🦴
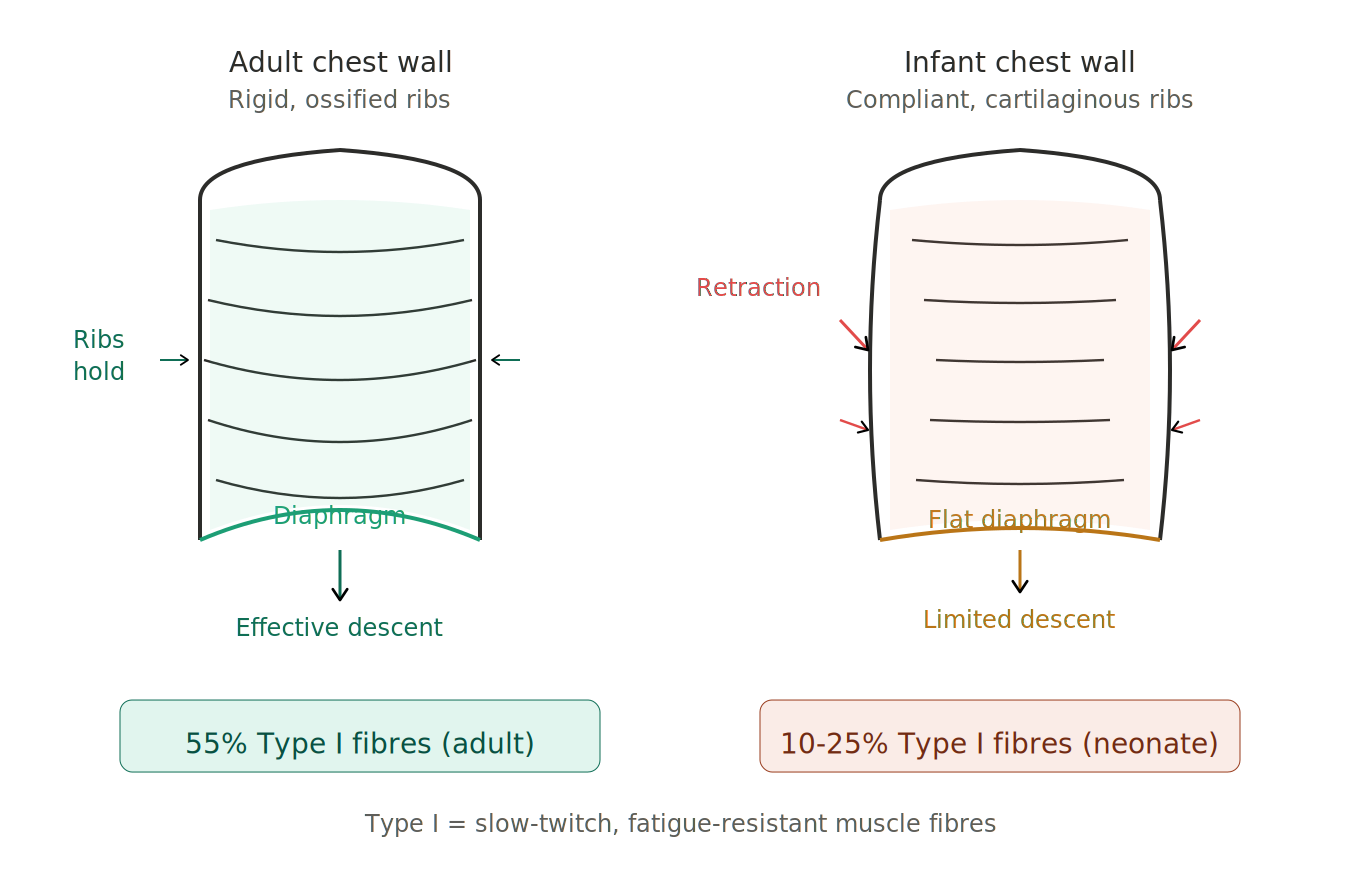
An adult rib cage is ossified and relatively rigid. It holds its shape under negative pleural pressure during inspiration. It does its job.
A neonate or infant rib cage? Cartilaginous. Highly compliant. And the ribs are oriented more horizontally. 😬
💡 What Actually Happens
When the diaphragm contracts and generates negative intrathoracic pressure, the compliant chest wall gets sucked inward instead of holding its shape.
This is chest wall retraction and it means the infant is wasting diaphragmatic work on deforming its own rib cage rather than inflating the lungs.
The infant is literally fighting its own chest wall to breathe. 😩
🪣 The Missing Bucket Handle
The diaphragm is also at a mechanical disadvantage. The ribs insert more horizontally, so the “bucket handle” effect that adults rely on for expanding thoracic volume is minimal in infants.
💪 The Diaphragm Fatigues Fast
This is the part that really gets you. ⚡
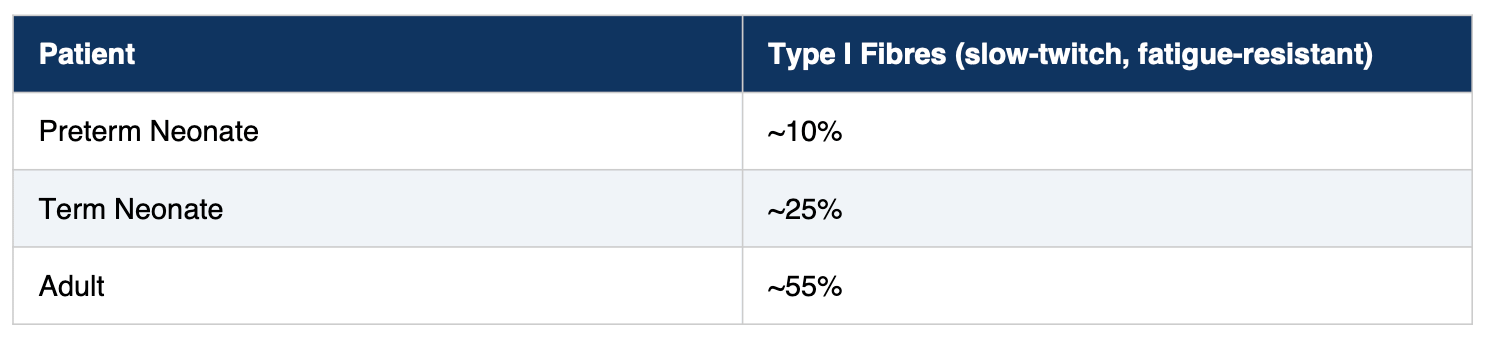
The infant diaphragm fatigues much faster. And once that diaphragm fatigues? There is very little accessory muscle reserve to compensate. The tank is empty. 🪫
🎯 Clinical Pearl
An infant in respiratory distress who is retracting heavily is telling you their system is failing at the mechanical level. They cannot sustain that work. Waiting for blood gas deterioration means you have waited too long. By the time the gas tells you there is a problem, the child has been losing the fight for a while. Act on clinical signs. Not numbers. 🚨
3️⃣ Oxygen Consumption Is Double 🔥
Here is a number that should change how you behave during every paediatric intubation:
That is a two-fold difference per kilogram. The engine is running hotter in kids. All the time. 🏎️💨
⏱️ The Brutal Consequence
The time from apnoea to desaturation is dramatically shorter.
90 seconds.
That is your entire window. From the moment ventilation stops to the moment the sats start crashing. There is no plateau. There is no grace period. 📉
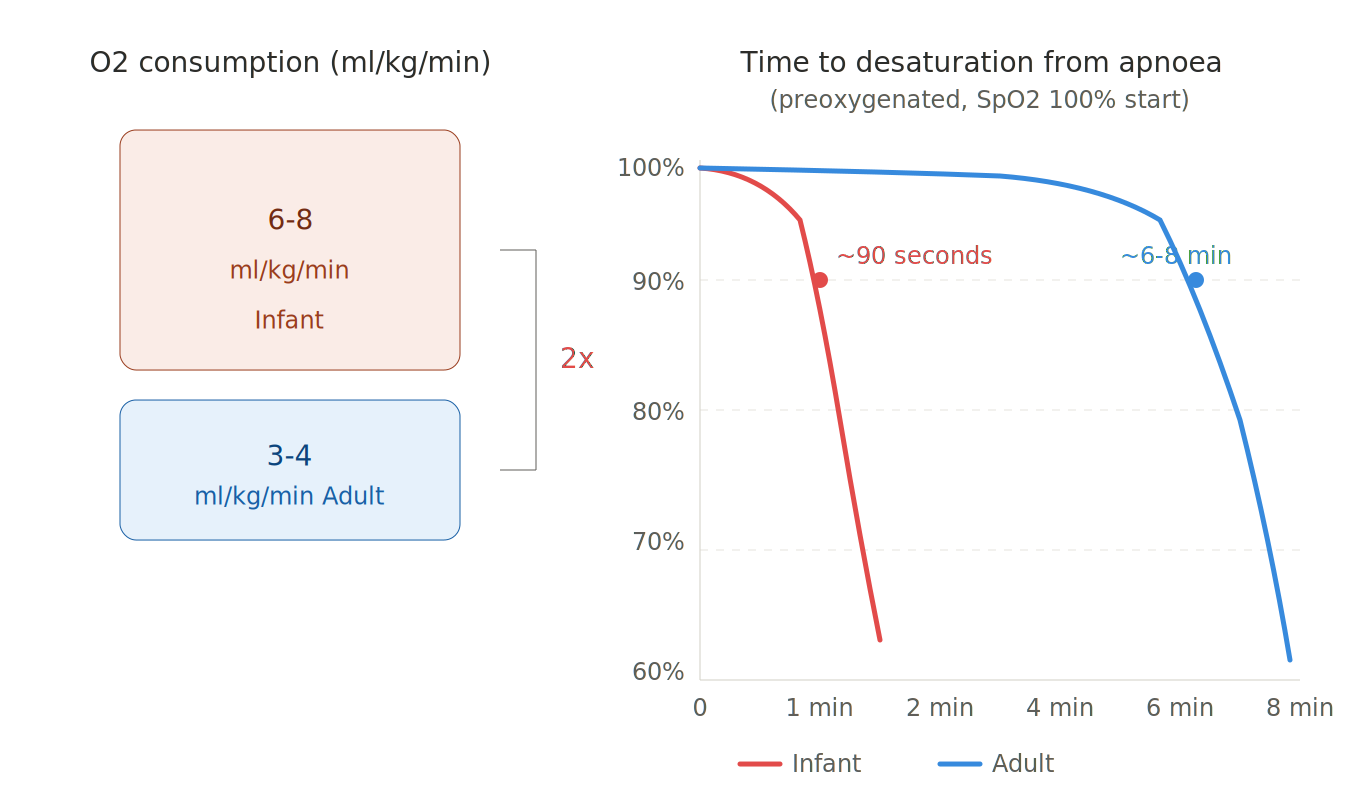
The metabolic rate is higher. CO₂ production is higher. The ventilatory demands relative to body weight are greater. The system is running at near-maximum capacity even at baseline.
🎯 Clinical Pearl
Paediatric intubation cannot be treated as a leisurely procedure. You preoxygenate. You have your plan, your backup plan and your equipment ready. There is no time for troubleshooting mid-attempt. First-pass success is not a flex. It is a physiological necessity. 🎯
4️⃣ FRC Is Dangerously Close to Closing Capacity 💨
This is the one that catches people out. It is the most conceptually tricky of the four but it might be the most clinically important.
📖 Definitions First
Functional Residual Capacity (FRC) = the volume of gas remaining in the lungs at the end of a normal passive exhalation. It is your oxygen reserve. It is also what keeps alveoli from collapsing between breaths.
Closing Capacity (CC) = the lung volume at which small airways begin to close during exhalation.
🧩 The Critical Relationship
In adults: CC sits well below FRC during tidal breathing. Airways remain open throughout the respiratory cycle. Comfortable margin. ✅
In neonates and infants: CC is at or above FRC. 😱
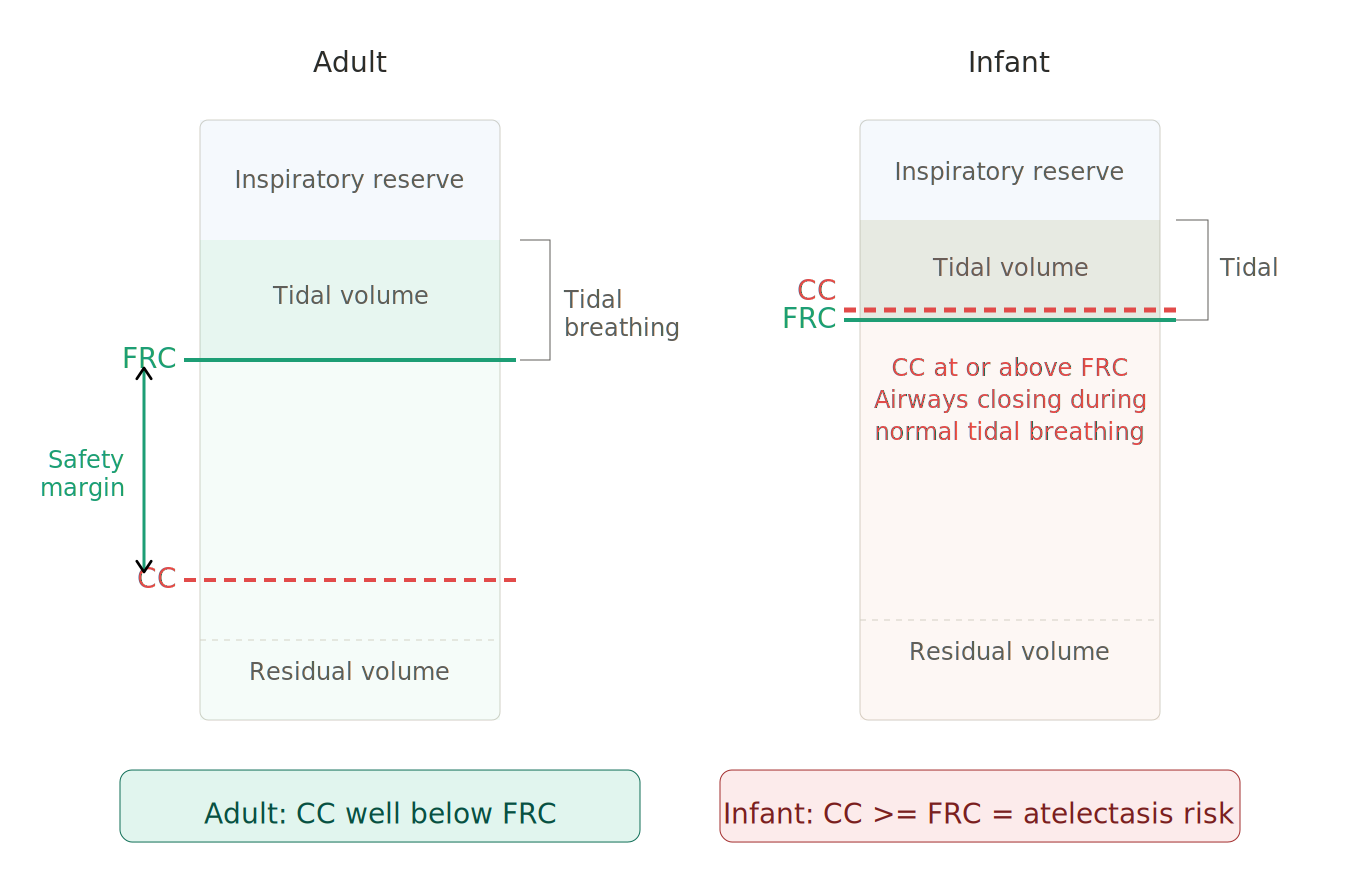
This means that during normal tidal breathing, small airways are closing and alveoli are collapsing with every single breath.
The infant is living on the edge of atelectasis at baseline. 🪨
Now add anything that further reduces FRC:
🛏️ Supine positioning
🫃 Abdominal distension
💊 General anaesthesia
💉 Muscle relaxation
🌬️ Positive pressure ventilation with inadequate PEEP
...and you push the patient into frank airway closure and shunt.
🎛️ This Is Why PEEP Matters So Much
PEEP is not optional in paediatric ventilation. It is the thing keeping small airways open.
But it is a tightrope:
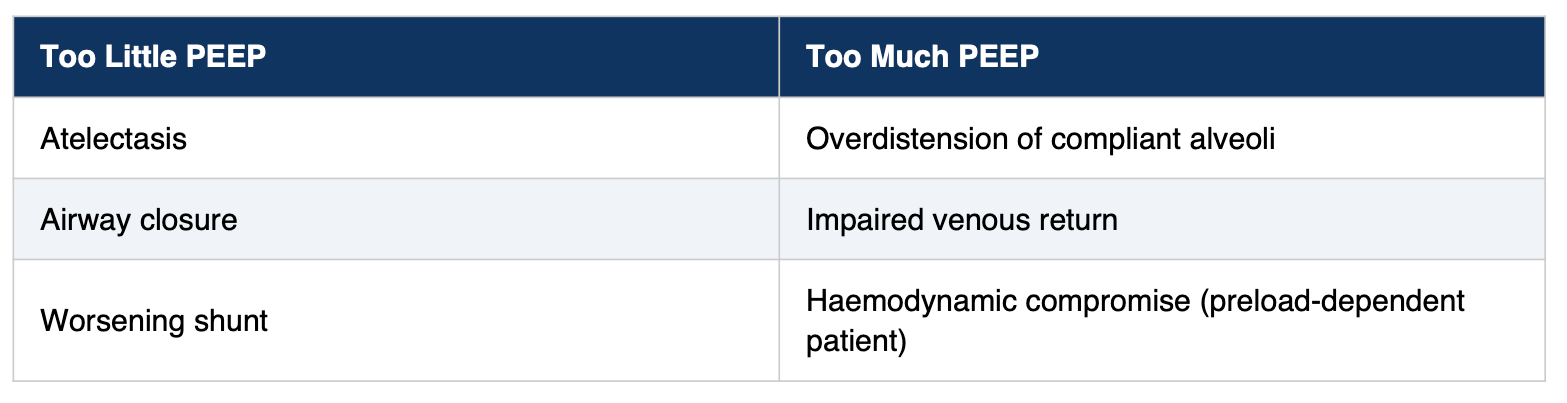
🎯 Clinical Pearl
PEEP is non-negotiable. Recruitment is an active process. Anything that reduces FRC (positioning, abdominal pathology, anaesthesia) will cause immediate clinical deterioration. Set it. Respect it. Monitor it. Don’t wing it. 🎚️
🧵 Pulling It All Together: A Cheat Sheet
These four physiological facts drive almost every decision in paediatric ventilation. Here is what each one is telling you at the bedside:
🔺 Airway Geometry Says...
Tube sizing is critical
Cuffed tubes need careful pressure monitoring
Post-extubation stridor is a real and predictable threat
A half-size-too-large tube → subglottic injury
A half-size-too-small tube → unacceptable leak
🦴 Chest Wall Compliance Says...
The infant cannot generate or sustain the work of breathing you might tolerate in an adult
Early intervention matters
Waiting for exhaustion is not a strategy
🔥 Oxygen Consumption Says...
Apnoeic windows are measured in seconds, not minutes
Preoxygenation buys you less time than you think
Every failed intubation attempt carries a higher cost
💨 FRC Physiology Says...
PEEP is non-negotiable
Recruitment is an active process
Anything that reduces FRC will cause immediate clinical deterioration
⚡ The Bottom Line
Paediatric patients have less reserve, less margin and less time.
If you approach them with the same timeline and the same thresholds you use in adult practice, you will be too late.
Every second counts. Every millimetre counts. Every cmH₂O of PEEP counts. 🫁
🔜 Next in the Series
Part 2: Modes of Ventilation in Paediatrics
Pressure control vs volume control, when SIMV still has a role and why HFOV exists.
Stay tuned. 👀
Spoon Fed PEM: bite-sized, high-yield paediatric emergency medicine education.
If you found this useful, share it with a colleague who needs it. 🩺💛