
Thymus or Pathology? The CXR Trap That Catches Everyone
A practical framework for reading the paediatric chest X-ray with confidence

The scenario: A 6-week-old infant with mild wheeze and tachypnoea. The CXR shows a large white opacity in the superior mediastinum spilling into the right hemithorax. Do you call it consolidation? A mass? Or a perfectly normal thymus? This one distinction determines whether a child gets admitted, irradiated or sent home safely.
🧠 Why This Is a Real Problem
The normal thymus is the single most misidentified structure on paediatric chest radiographs. It is large, it is anterior and it sits exactly where pathology likes to hide. Miss it in one direction and you have an unnecessarily admitted infant with a battery of investigations. Miss it in the other direction and a mediastinal mass walks out the door.
The good news is that the thymus is generous with its clues. Once you know the signs, they are hard to unsee.
The thymus is soft. Pathology is not.
This single fact explains almost every distinguishing sign on the CXR.
📅 Know Your Age Window First
The thymus is only a diagnostic problem in the first few years of life. After that it involutes, becomes fatty and disappears from the film.
🔵 0 to 2 years: Thymus largest relative to body size. Most prominent and most commonly misread.
🟡 2 to 5 years: Visible but less prominent. Still a relevant differential.
⚪ After puberty: Involuted. An anterior mediastinal opacity now is NOT normal thymus.
⚠️ AGE RULE
If a child is over 6 and you are seeing an anterior mediastinal opacity, stop calling it thymus. Think lymphoma, teratoma or thymoma until proven otherwise.
⛵ The Four Classic Signs
⛵ Sail Sign
The right lobe projects laterally and inferiorly forming a triangular opacity like a sail. Inferior angle points inferolaterally. Your most important clue.
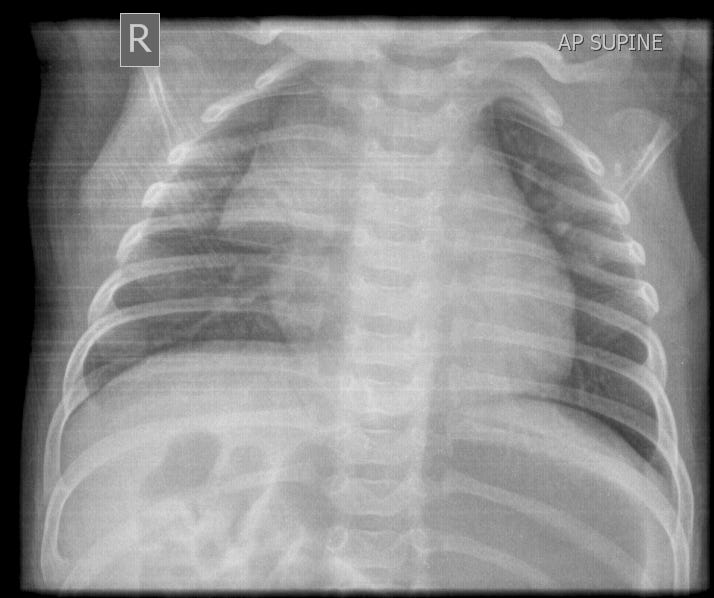
⛵ Sail Sign — Radiopaedia Teaching CaseClassic triangular right-sided thymic opacity with convex lateral border and inferolateral apex in an infant.
View on Radiopaedia: Thymic Sail Sign→
🌊 Wave Sign
Anterior ribs indent the pliable thymus creating a scalloped lateral border. Only a soft structure deforms around ribs. Consolidated lung and masses do not.
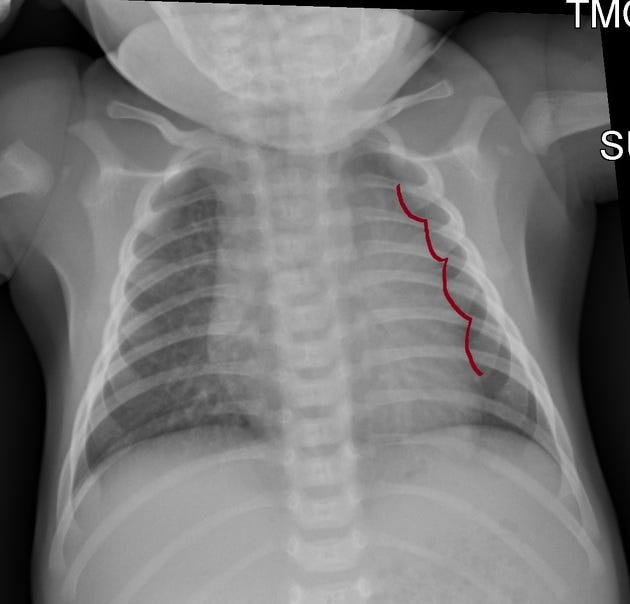
🌊 Wave Sign — Radiopaedia Teaching CaseScalloped lateral border of the thymus produced by anterior rib indentation. Diagnostic of a pliable soft-tissue structure.
View on Radiopaedia: Thymic Wave Sign→
🔔 Notch Sign
A step at the junction of the thymic shadow and cardiac silhouette on the frontal view. Separates thymus above from heart below.
👁️ See-Through Sign
Pulmonary vascular markings remain visible through the thymic opacity. Consolidation obliterates them. The thymus does not.
📐 Always Get a Lateral View
If the frontal view is ambiguous, the lateral CXR will usually resolve the question.
✅ Normal thymus fills the anterior retrosternal space
✅ The posterior clear space is preserved — thymus does not extend behind the heart
✅ Trachea is not displaced posteriorly
❌ Posterior mediastinal extension = not normal thymus
📐 Lateral CXR — Normal Thymic ShadowThymus confined to the anterior mediastinum with clear posterior space preserved and no tracheal displacement.
View on Radiopaedia: Normal Lateral Thymic Shadow→
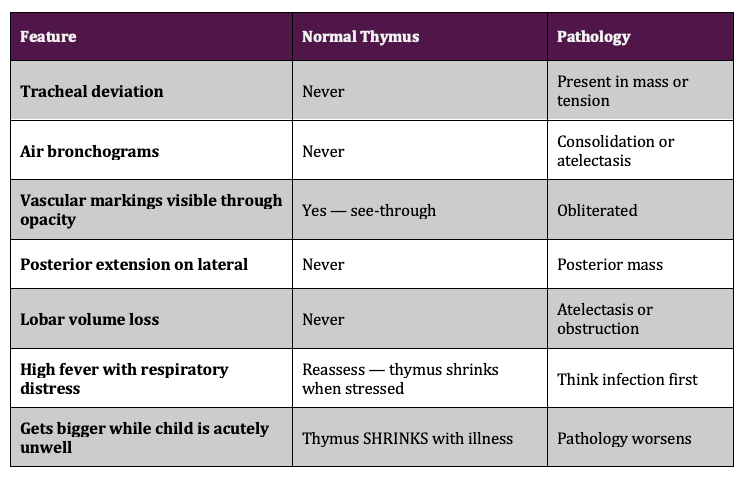
🚩 Red Flags — This Is NOT Thymus
🔄 The Thymic Rebound Phenomenon
This one catches experienced clinicians.
The thymus undergoes acute stress involution during illness, surgery or steroid exposure. On recovery, it rebounds and can appear larger than before.
Classic scenario: a child completes chemotherapy. Follow-up CXR shows a large anterior mediastinal opacity. Relapse? No. Rebound thymic hyperplasia — and it is actually a good sign.
✅ REBOUND RULE
If an opacity appears or enlarges on a recovery CXR after illness or chemotherapy and has classic thymic morphology, this is rebound. Do not escalate without specialist input.
🔄 Thymic Rebound — Radiopaedia Teaching CaseThymus enlarges dramatically after recovery from illness or completion of chemotherapy. Easily mistaken for relapse.
View on Radiopaedia: Thymic Rebound→
🧩 5-Step Bedside Framework
1 Age check
Under 5 years? If not, thymus is not your answer.
2 Look for the sail sign
Triangular right-sided opacity with inferolateral apex. Present = strongly favour thymus.
3 Look for the wave sign
Scalloped lateral border from rib indentation. Present = almost certainly thymus.
4 Get the lateral view
Posterior clear space preserved? No posterior extension? No tracheal displacement? = Thymus confirmed.
5 Clinical overlay — non-negotiable
Well child with mild symptoms = reassure and discharge. Unwell child with high fever or distress = treat for pathology and re-image at 24 to 48 hours regardless of what the film shows.
✅ Bottom Line
What to take into your next shift
🔵The normal thymus is visible and prominent in children under 5
⛵Sail sign and wave sign are your primary tools. Learn them cold.
📐The lateral view is not optional when the diagnosis is in doubt
✋No mass effect, no air bronchograms, no tracheal shift = thymus until proven otherwise
🔻The thymus shrinks with stress and illness. Growing while the child is acutely unwell = not thymus.
🔄Thymic rebound after recovery or chemotherapy can be dramatic. Do not panic.
🚨A sick child with a mediastinal opacity always needs clinical correlation. Radiology does not trump the bedside.
REFERENCES
Donnelly LF et al. Diagnostic Imaging: Pediatrics. Elsevier.
Swischuk LE. Emergency Imaging of the Acutely Ill or Injured Child, 4th Ed. Lippincott Williams and Wilkins.
Radiopaedia.org — Thymic sail sign, wave sign, notch sign, thymic rebound. radiopaedia.org