
🧠 The 3AM Headache: A Spoonfed Approach to the Undiagnosed Nontraumatic Headache in Children
Because “Mum, my head hurts” sits on a spectrum from “give paracetamol and go back to sleep” to “call the neurosurgeon now” and your job at 3AM is to know which one you are looking at. 🚨


It is 3AM. A 7 year old is wheeled into your ED. Mum is exhausted. The triage note says “headache x 2 days.” The child is quiet, curled up, keeping the lights off with one hand over the eyes.
Two doors down there is another 7 year old with a headache. Same triage note. This one is chatty, eating crisps, watching cartoons on a phone at full brightness.
Same complaint. Wildly different stories. One of these might have a bleed. One of these needs paracetamol and a dark room. The whole game tonight is telling them apart without CT scanning every child who walks through the door.
Here is the uncomfortable truth this article is built on: the eye does not see what the mind does not know. If you do not carry the differential in your head, you will not spot the red flag sitting in front of you. So let us load the differential first, then go back to the history and examination knowing exactly what we are hunting for. 🎯
📊 The Spectrum: Three Tiers
Everything that causes a nontraumatic headache in a child fits into a pyramid. Most of what you see lives at the bottom. What can kill lives at the top. Your brain needs both loaded at once.
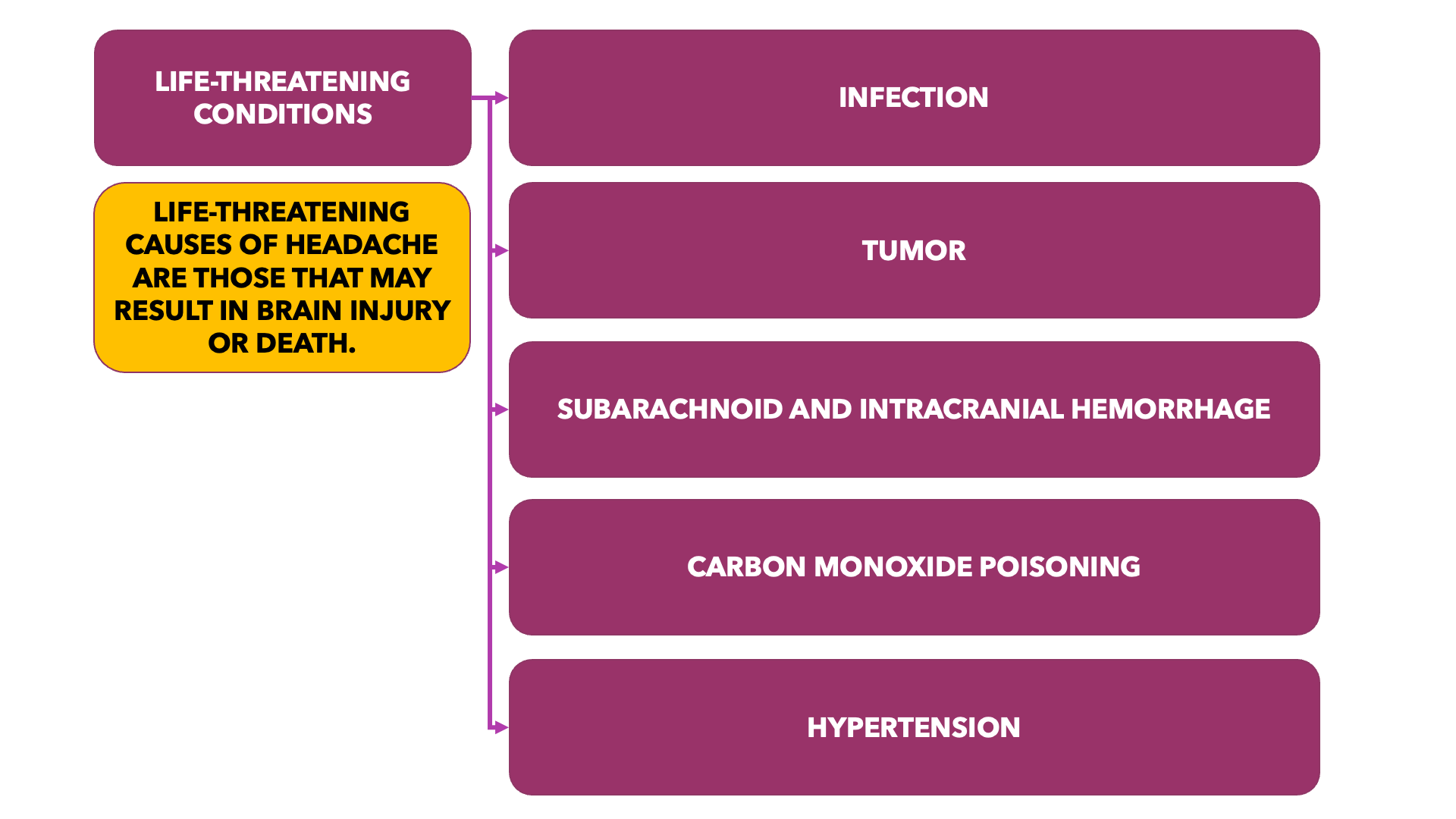
🔴 TIER 1 ➜ LIFE-THREATENING (rare but lethal)
▪️Infection (meningitis, encephalitis, abscess)
▪️ intracranial haemorrhage
▪️ CO poisoning
▪️ tumour
▪️ malignant hypertension
🟣 TIER 2 ➜ OTHER CONDITIONS (uncommon)
▪️Idiopathic intracranial hypertension
▪️ TMJ dysfunction
▪️ cluster headache
🔵 TIER 3 ➜ COMMON (the overwhelming majority)
▪️Viral illness with fever
▪️ migraine
▪️ tension-type headache
▪️ sinusitis
▪️ pharyngitis
▪️ otitis media
Clinical pearl: The current PECARN and AAN framing is that roughly 0.5% to 1% of children presenting to the ED with headache have an emergent intracranial abnormality such as a tumour, haemorrhage, or stroke.
Yet more than a third get scanned.
The mission is to shrink that gap without missing the 0.5% to 1%. 🎯
🔴 TIER 1: The Stuff That Can Kill
Life-threatening causes of headache are those that may result in brain injury or death. In younger children, especially those who cannot describe their symptoms, the signs can be brutally subtle.
🦠 Infection
Children with a life-threatening infection almost never have headache in isolation. Look for the company it keeps: altered mental status or focal neurologic findings.
Bacterial meningitis 🧫
The classic picture is the irritable or lethargic child with fever plus neck pain, stiffness, or headache.
Incidence has dropped since routine Hib (2, 3, 5 and 18 months) and pneumococcal vaccination. Do not let that lull you. Undervaccinated and partially vaccinated children still present.
Viral encephalitis 🧠
Progressive fever and headache plus abrupt altered sensorium (bizarre behaviour or hallucinations).
In previously healthy kids, HSV causes roughly 10 to 20% of sporadic encephalitis and it is the one treatable pathogen. Miss it and you miss your window with aciclovir.
Arboviruses matter too (eg Japanese encephalitis, dengue, West Nile depending on region). Take a travel history.✈️
Orbital or cerebral abscess 👁️

Focal infections give focal signs on ocular and/or neurologic examination.
Cerebral abscess and cerebral venous thrombosis are uncommon but life-threatening complications of orbital, sinus, ear, and dental infections.
Higher risk in immunocompromise and congenital heart disease with right-to-left intracardiac shunting.
🩸 Subarachnoid and Intracranial Haemorrhage
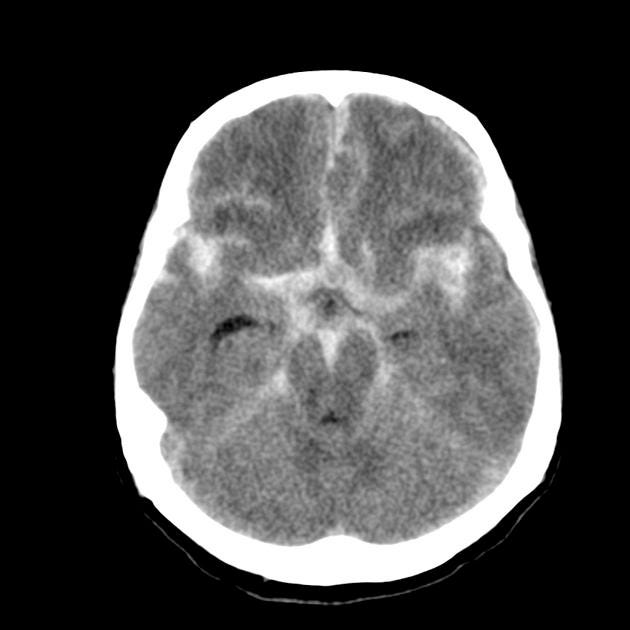
Abrupt onset headache reaching maximal intensity in under one minute (thunderclap).
May come with hemiparesis and seizures.
Sickle cell disease is a big one: roughly 1 in 3 headaches in sickle cell children are actually bleeds. Do not treat that headache as routine. 🚩
💨 Carbon Monoxide Poisoning
Symptoms of mild to moderate CO poisoning are nonspecific and headache is prominent.
Occult sources: improperly vented heaters, space heaters, automobile exhaust fumes, and house fires. 🔥
The tell: multiple family members from the same household with headache. If the whole family is symptomatic, think CO, not a virus. A single family unit presenting together is a screaming red flag.
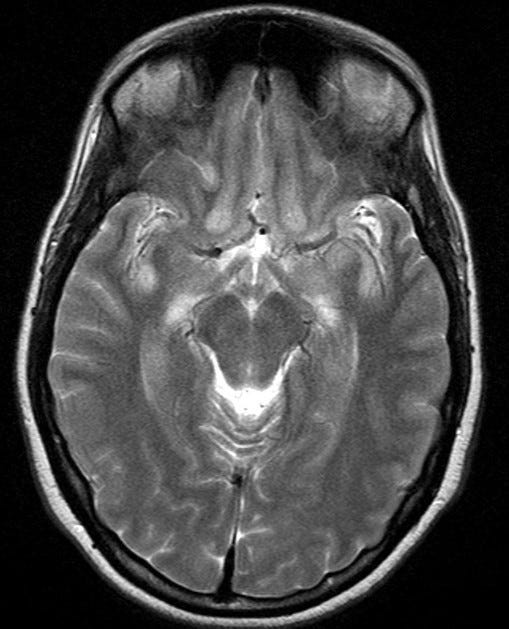
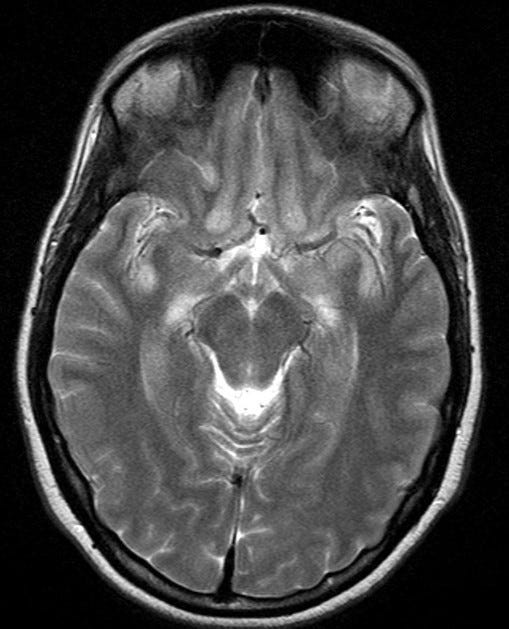
🎗️ Brain Tumour
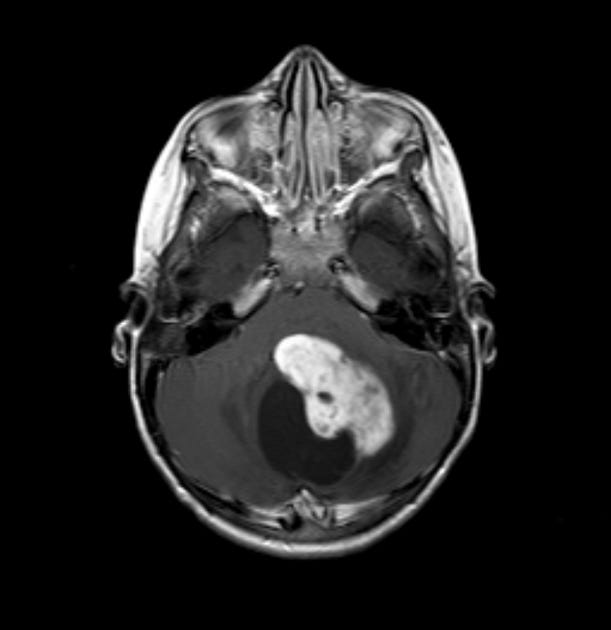
Chronic progressive headache (increasing frequency and severity over time) is the classic presentation.
Reassuring reality: fewer than 3% of children presenting to the ED with headache have a newly diagnosed brain tumour.
Early symptoms are nonspecific and diagnosis is often delayed. But at the point of diagnosis, the overwhelming majority of these children have other symptoms alongside the headache. Isolated headache with a normal exam is rarely a tumour.
🩺 Hypertension
Hypertensive crisis can present as headache from hypertensive encephalopathy.
Look for visual changes (retinal haemorrhage or exudates), altered mental status, and seizures.
In children, hypertensive encephalopathy is uncommon and usually driven by systemic illness or renovascular disease, not primary hypertension.
Phaeochromocytoma is exceptionally rare but presents with the memorable quartet: headache, pallor, diaphoresis, and hypertension. 💦
Actually measure the blood pressure. With the right cuff size. It is the single most skipped vital in a headache workup.
🔵 TIER 3: The Common Stuff (Where Most of Your Night Lives)
🤒 Infection with Fever
Children with fever, almost always from infection, frequently complain of headache.
The mechanism is vasodilation. Treat the fever, treat the source, the headache usually follows.
🦠 Viral Meningitis
A typical presentation in older children and adolescents.
Hunt for virus-specific clues: rash or mouth lesions point to enterovirus.
😷 Pharyngitis
Headache, sore throat, and abdominal pain are the classic triad of streptococcal pharyngitis.
Influenza mimics it and adds headache to the mix.
👂 Other Infections
Otitis media, sinusitis, and dental infections all cause headache.
Localised pain plus signs of inflammation give you the diagnosis at the bedside.
🌩️ Migraine
In EDs presenting with acute headache, migraine is second only to viral illness as the primary cause.
Typically recurrent and episodic with a pattern parents can describe in their sleep.
The red flag inside migraine: any child with a significant change in the quality, severity, or timing of a known headache pattern needs re-evaluation for another cause. Do not anchor on “known migraineur.”
Features of migraine in children (how paeds differs from adults): 👇
Attacks last 2 to 72 hours (adults: 4 to 72). This paediatric duration is the ICHD-3 modification for under-18s.
Headache is more often bilateral in children. The adult unilateral pattern emerges in late adolescence or early adulthood.
Photophobia and phonophobia can be inferred from behaviour in young children (turning off the lights, hiding under a blanket).
📋 ICHD-3: Migraine Without Aura
A ➜ At least five attacks fulfilling B through D
B ➜ Headache attacks lasting 4 to 72 hours untreated (2 to 72 hours in children and adolescents under 18)
C ➜ At least two of: unilateral location ▪️ pulsating quality ▪️ moderate or severe intensity ▪️ aggravation by or avoidance of routine physical activity
D ➜ During headache at least one of: nausea and/or vomiting ▪️ OR photophobia and phonophobia
E ➜ Not better accounted for by another ICHD-3 diagnosis
📋 ICHD-3: Migraine With Aura
A ➜ At least two attacks fulfilling B and C
B ➜ One or more fully reversible aura symptoms: visual ▪️ sensory ▪️ speech/language ▪️ motor ▪️ brainstem ▪️ retinal
C ➜ At least three of six: aura spreads gradually over ≥5 min ▪️ two or more symptoms in succession ▪️ each symptom lasts 5 to 60 min ▪️ at least one symptom unilateral ▪️ at least one symptom positive ▪️ aura accompanied or followed within 60 min by headache
D ➜ Not better accounted for by another ICHD-3 diagnosis
😣 Tension-Type Headache
The International Headache Society term for what used to be called tension, muscle-contraction, stress, or psychogenic headaches.
Occurs in 10 to 25% of schoolchildren and adolescents, making it about as common as migraine.
In children it associates with depression, oromandibular dysfunction, and muscle tension from stress.
The key contrast with tumour: pain is intermittent, recurring, but nonprogressive, and the neurologic exam is unremarkable.
🟣 TIER 2: The In-Between
🦷 Temporomandibular Joint (TMJ) Dysfunction
Occurs in children with primary and mixed dentition.
Increased pain while chewing plus point tenderness over the mandibular condyle.
Headache is more frequent among older children.
🧠 Idiopathic Intracranial Hypertension (IIH)
The classic pentad:
Papilloedema 👁️
Increased ICP
Normal CSF content
Normal neuroimaging
Absence of neurologic signs except cranial nerve VI palsy
No known cause
Who gets it: headache is the most common complaint in children old enough to describe it. Most patients are adolescents and typically female. 🚩 Check the fundi. Every time.

👁️ Trigeminal Autonomic Cephalalgia (Cluster Headache)
The most common trigeminal autonomic cephalalgia.
Unilateral, frontal-periorbital, severe, lasting under three hours, but occurring in tight “clusters” over a short period.
Mostly presents between ages 10 and 20.
Look for ipsilateral autonomic findings: lacrimation, rhinorrhoea, ophthalmic injection, and sometimes Horner syndrome (ipsilateral miosis, ptosis, facial anhidrosis).

🔍 Now Go Back to the History
Now that you know what you are looking for, the history stops being a checklist and becomes a hunt.
👶 Patient Age
Headaches in children younger than six are more likely to have an underlying cause, most commonly a febrile viral illness. Young age plus headache should lower your threshold to look harder.
⏱️ Mode of Onset
Thunderclap (”worst headache of my life,” maximal in under a minute) raises intracranial haemorrhage from AVM or aneurysm.
But in isolation, without neck pain or stiffness, thunderclap is nonspecific in children. Context matters.
🕐 Timing
Tension-type headaches develop late in the day and rarely wake a child from sleep.
🛏️ Positional
A headache that presents or worsens on lying down, wakes the child from sleep, or hits soon after waking should raise concern for increased ICP or a space-occupying lesion, especially when paired with morning vomiting. 🚩🚩
📈 Severity and Quality
Less useful in young children than in adults.
Use sleep disturbance as a proxy for severity when the child cannot articulate it.
🗺️ If the Child Can Describe It
Laterality: unilateral suggests migraine or focal infection (sinusitis).
Location: cluster headaches are usually temporal or retro-orbital.
🔄 Pattern of Previous Headaches (The Money Framework)
1️⃣ ACUTE ➜ single episode, no prior history ➜ think viral illness
2️⃣ ACUTE RECURRENT ➜ consistent features, easily described ➜ think migraine
3️⃣ CHRONIC PROGRESSIVE ➜ increasing frequency and severity over time ➜ 🚩 think brain injury / haemorrhage / SOL
4️⃣ CHRONIC NON-PROGRESSIVE ➜ frequent, persistent, unchanged in character ➜ think tension headache
Pattern 3 is the one that should make your stomach drop. 🚨
🚩 Associated Symptoms to Actively Ask About
Fever · neck pain · altered mental status · localised pain · trauma · environmental exposure · changes in visual acuity · autonomic symptoms · aura.

📁 Past Medical History That Changes the Game
Malignancy · coagulopathy · sickle cell disease · cyanotic heart disease. Each one moves a “probably benign” headache up the pyramid.
🩺 The Examination (Where the Diagnosis Usually Hides)
👀 General Appearance
Most children with a serious cause look ill or have altered mental status (confused, lethargic, or comatose). The well-appearing, interactive child is your reassurance, not your CT scanner.
👂 Head and Neck
Examine to rule out trauma, then hunt for the source:
Otitis media on otoscopy
Sinusitis: facial tenderness or purulent rhinorrhoea
Strep pharyngitis: tonsillar swelling, erythema, exudate
Teeth and gingiva: inflammation or abscess
TMJ / masseter tenderness: TMJ dysfunction
Nuchal rigidity: migraine, meningitis, or intracranial haemorrhage
🖐️ Skin

Neurocutaneous syndromes (neurofibromatosis, tuberous sclerosis) carry brain-lesion risk. Look for café-au-lait spots and ash-leaf macules.
Bruising in a suspicious distribution raises non-accidental injury. Do not skip the skin. 🚩
🧠 Neurologic Examination (Non-Negotiable)
The majority of children with a serious neurologic cause have abnormalities on neuro exam. This is your highest-yield test and it costs nothing.
Altered mental status: encephalitis, haemorrhage, elevated ICP, hypertensive encephalopathy.
Focal or prolonged-postictal seizures: intracranial focus (haemorrhage, tumour).
Extraocular palsies or nystagmus: elevated ICP or mass compression.
Motor asymmetry, gait disturbance, poor fine motor coordination: focal intracranial lesion.
⚠️ Trap: some children with migraine develop focal deficits (ophthalmoplegia, motor weakness, ataxia). Usually caretakers can confirm this is the child’s typical pattern. First-ever focal deficit is not migraine until proven otherwise.
🔦 Fundoscopy
Do it on every child being evaluated for headache.
Hard in young or uncooperative patients, but try.
Papilloedema, haemorrhages, exudates, and abnormal vessels are markers of serious intracranial pathology.
🖥️ Imaging: When to Pull the Trigger
✅ SCAN when any of these are present:
🚩 Focal or gross neurologic deficit: cranial nerve deficit, visual field cut, focal motor weakness, asymmetric reflexes, focal seizure (beyond simple febrile), prolonged altered mental status (>60 min), ataxia, or dysmetria.
🚩 Papilloedema or other signs of raised ICP: headache precipitated or worsened by prolonged lying down (especially with vomiting), hypertension with brady- or tachycardia, or progressive vomiting.
🚩 Thunderclap / “worst headache”, especially with neck pain or stiffness.
🛑 DO NOT scan when:
Nontraumatic headache + no worrisome features + normal fundoscopy + normal neuro exam.
This group has a very low risk of a life-threatening intracranial abnormality. \
These patients do not require imaging. Radiation and sedation are not free. 📉
💉 Lumbar Puncture: When and How
LP is indicated when:
Suspected non-focal infection (meningitis, encephalitis) 🦠
Concern for subarachnoid haemorrhage not diagnosed on neuroimaging
Measuring opening pressure for suspected IIH (after neuroimaging)
Critical safety point ⚠️: Patients with a focal neuro exam or significant concern for raised ICP / papilloedema need an emergency CT or fast MRI before LP because of herniation risk.
Send the right tubes: CSF cell count and differential, glucose, protein, Gram stain, and bacterial culture. Add opening pressure when IIH is on the table.
🧭 The Diagnostic Algorithm
“Worst headache of life” / thunderclap?
Yes → work up for subarachnoid haemorrhage / vascular cause.
No → next question.
History of chronic or recurrent headaches?
Yes → typical pattern with no new findings? → migraine / tension / chronic daily headache.
No, or new findings → next.
Focal neuro exam OR signs of raised ICP (papilloedema; hypertension with brady/tachycardia and progressive vomiting; headache worse lying down, especially with vomiting)?
Yes → neuroimaging.
Acute process on imaging → tumour, mass, hydrocephalus, SAH/vascular cause.
No acute process → focal findings >60 min → migraine variants (prolonged aura, hemiplegic, cerebrovascular, Todd’s). Otherwise → LP with opening pressure → interpret CSF (RBCs → SAH; WBCs → meningitis/encephalitis; raised opening pressure → IIH or cerebral venous thrombosis; normal → pseudopapilloedema).
No → Fever?
Yes → meningeal signs? → CSF abnormal → meningitis. Otherwise viral syndrome / sinusitis / dental abscess.
No → other history/exam abnormal? → exposure (CO poisoning), raised BP (hypertension), focal tenderness (sinus/dental abscess, TMJ). Otherwise migraine / tension headache.
🎯 The Bottom Line
The differential is your safety net. Load it before you walk into the room. The eye does not see what the mind does not know.
Isolated headache with a normal neuro exam, normal fundoscopy, and no red flags is reassuring and does not need a CT. Roughly 99% of these children are fine, and radiation is not benign.
The red flags that should stop you cold: thunderclap with neck stiffness, morning headache with vomiting, headache worse lying down, chronic progressive pattern, focal neuro deficit, papilloedema, age under 6, and the child who simply looks unwell.
Special populations move the needle: sickle cell (1 in 3 headaches are bleeds), the whole family symptomatic (CO poisoning), immunocompromise and cyanotic heart disease (abscess).
Fundoscopy and a proper neuro exam are your two highest-yield, zero-cost investigations. Do them every single time.
📚 References
Bachur RG, Shaw KN. Fleisher & Ludwig’s Textbook of Pediatric Emergency Medicine. Lippincott Williams & Wilkins, 2015.
Saladino RA. Emergency department approach to nontraumatic headache in children. UpToDate.
Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018; 38(1): 1-211.
Lewis DW, Ashwal S, Dahl G, et al. Practice parameter: Evaluation of children and adolescents with recurrent headaches. Neurology 2002; 59: 490.
Massano D, Julliand S, Kanagarajah L, et al. Headache with focal neurologic signs in children at the emergency department. J Pediatr 2014; 165: 376.
Papetti L, Capuano A, Tarantino S, et al. Headache as an emergency in children and adolescents. Curr Pain Headache Rep 2015; 19: 3.
Wilne S, Koller K, Collier J, et al. The diagnosis of brain tumours in children. Arch Dis Child 2010; 95: 534.
Seshia SS, Abu-Arafeh I, Hershey AD. Tension-type headache in children: The Cinderella of headache disorders. Can J Neurol Sci 2009; 36: 687.
Anttila P. Tension-type headache in childhood and adolescence. Lancet Neurol 2006; 5: 268.
Lewis DW. Pediatric migraine. Neurol Clin 2009; 27: 481.
PECARN. Stratification of risk for emergent intracranial abnormalities in children with headaches (study protocol). 2023.