
Pre-Intubation Optimisation - Don’t Kill Them On the Way In. 💀
Spoon Fed PEM | Paediatric Ventilation Series | Part 3


You’ve decided to intubate.
Good.
Now the uncomfortable bit: the act of intubating a sick child can kill them faster than the illness you are treating.
Peri-intubation cardiac arrest in children is not a freak event. It is a predictable consequence of putting a hypoxic, hypovolaemic, acidotic child to sleep and removing their own respiratory drive at the exact moment they can least afford it.
This post is about the minutes before you touch a laryngoscope. Get these right and the tube almost places itself. Get them wrong and you are running a code. 🚨
⚠️ Evidence note
Much of paediatric peri-intubation practice rests on physiological reasoning, observational data and extrapolation from adult and neonatal work rather than large paediatric RCTs. Treat the mechanisms and principles here as consensus- and physiology-based teaching. Defer to your local RSI and PICU guidelines for specific drugs, doses and flow settings. I have deliberately not stated fixed doses or flow rates, because these vary by protocol and a wrong number is dangerous.
⚠️ What actually kills them
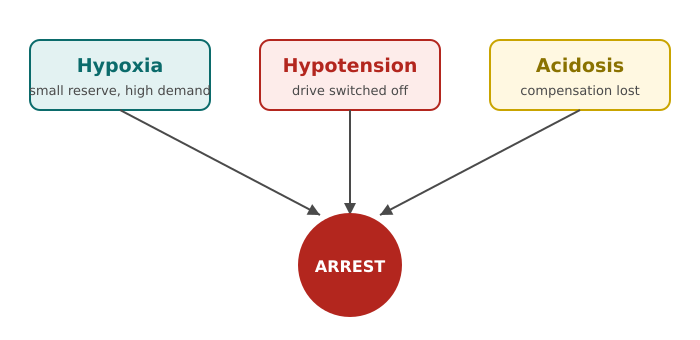
Three mechanisms. Learn them cold.
1️⃣ Hypoxia 🔵
Children desaturate fast. A small child has a small functional residual capacity (the oxygen reservoir left in the lungs after a normal breath out) and a high oxygen consumption per kilo. Small reservoir plus high demand means the safe apnoea window is short. You paralyse, you lose 30 seconds fumbling, and the SpO₂ is already falling hard.
Exact desaturation times vary widely by age, weight, lung pathology and pre-oxygenation quality. Any quoted “seconds to desaturation” figure is a rough teaching estimate, not a promise.
2️⃣ Hypotension and cardiovascular collapse 🩸
The sick child is often running on their own adrenaline. Their blood pressure is being propped up by sympathetic drive. Your induction agent switches that drive off. Positive pressure ventilation then drops venous return (the blood coming back to the heart) on top of it. The floor falls out.
3️⃣ Acidosis 🧪
A severely acidotic child compensates by breathing hard to blow off CO₂. The moment you paralyse them, that compensation stops. CO₂ climbs, pH drops further, and an already irritable heart arrests.
🫧 Apnoeic oxygenation: buy yourself time
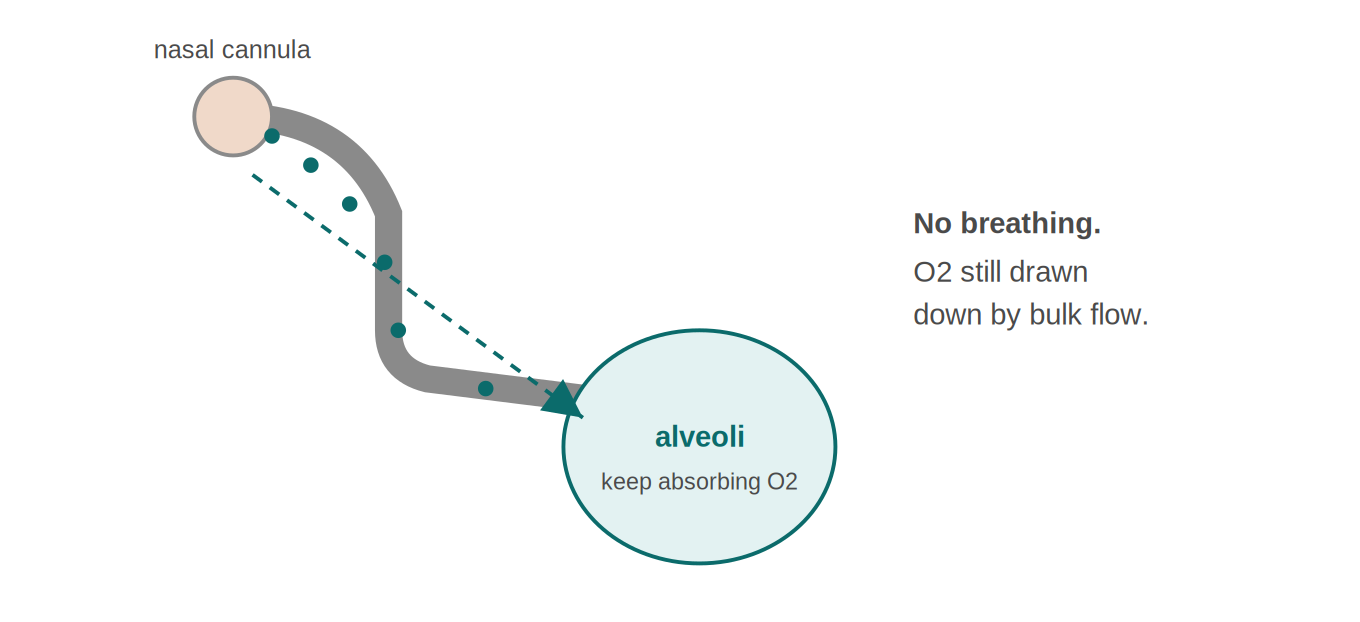
Core principle: even when the child is not breathing, the alveoli keep absorbing oxygen. If you keep oxygen flowing past the vocal cords, it is drawn down into the lungs by bulk flow. This stretches out the safe apnoea window.
How to do it 👇
🟢 Pre-oxygenate properly first. Aim for the highest SpO₂ you can get, for a few minutes if time allows. This washes nitrogen out of the lungs and fills the reservoir with oxygen.
🟢 Leave nasal cannulae on underneath your mask or NIV interface, and keep them running through the apnoeic period and the attempt itself.
🟢 Flow scales with size. [Inference] Precise flow settings are unit- and device-dependent and based on observed practice rather than a single fixed rule. Follow your local guidance.
⚠️ Apnoeic oxygenation buys time. [Inference] Based on the underlying physiology and observed practice, it delays desaturation rather than preventing it. It does not replace good pre-oxygenation or a fast, clean first attempt.
🧍 Positioning by age: geometry wins attempts
You cannot brute-force a bad view. Positioning is free and it works.
👶 Infants (roughly under 2)
Big occiput (the back of the head). Lie them flat and the head flexes forward, folding the airway shut. Fix it:
🔹 Shoulder roll to counteract the occiput and line the airway up.
🔹 Aim for a neutral to slightly extended head position, not the adult sniffing ramp.
🔹 Ear-to-sternal-notch is the target sightline.
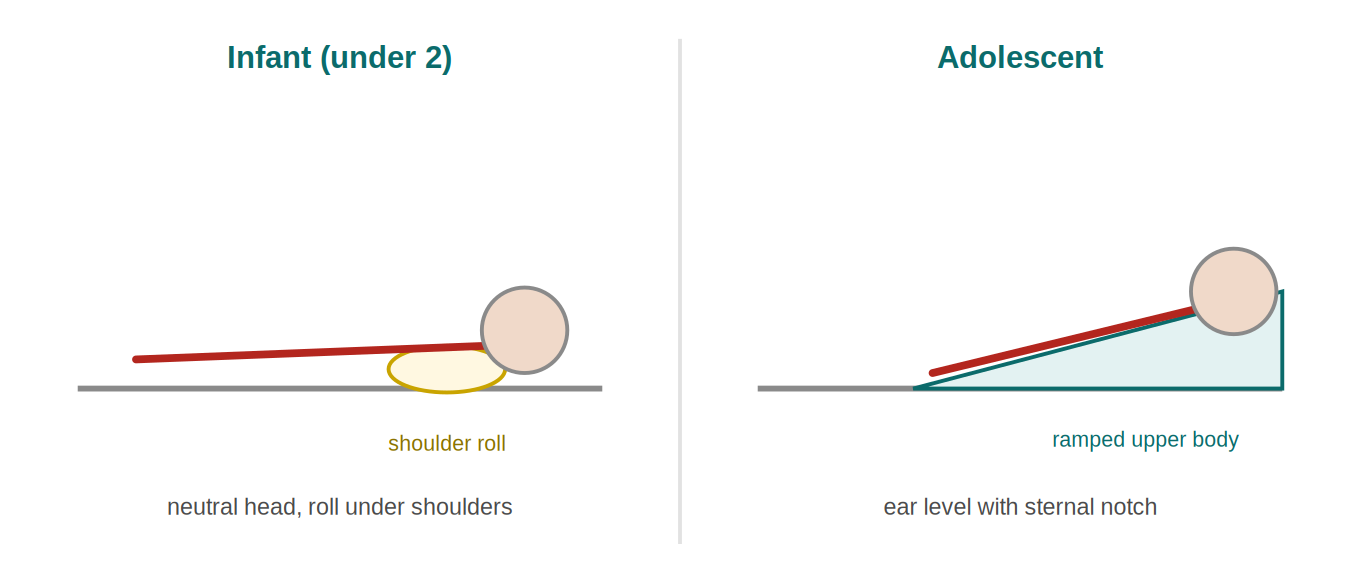
🧒 Older children and adolescents
🔹 The adult sniffing position increasingly works: neck flexed on body, head extended on neck.
🔹 In bigger or heavier adolescents, ramp the upper body so the ear sits level with the sternal notch. This also improves pre-oxygenation.
🩺 Haemodynamic preparation: fix the circulation first
This is the step people skip and it is the one that kills.
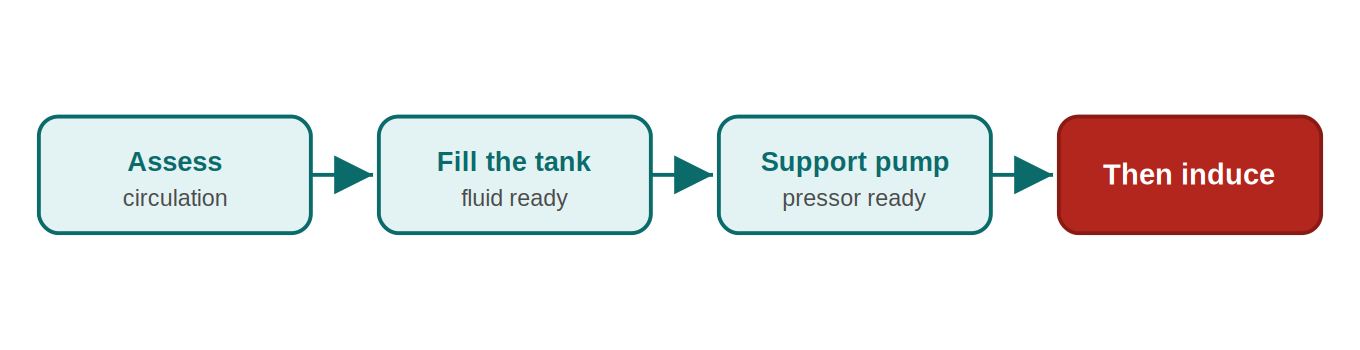
Before induction, ask: fluid-down, pressure-down, or both? 🤔
💧 Volume: if they are dry or septic, get fluid in or at least have it running and ready. Hypovolaemic child plus induction agent equals collapse.
💉 Vasopressors ready: have a push-dose or peripheral infusion drawn up and in your hand or running before you induce any child you think is fragile. Reaching for it after the arrest is too late.
❤️ Choose the agent for the haemodynamics. [Inference] Agent choice and dosing are context- and guideline-specific. The general principle from observed practice is to favour agents with a smaller cardiovascular hit and to reduce dose in the shocked child. Follow your local RSI guideline for the actual drugs and doses.
🚩 Resuscitate before you intubate. If you have time to optimise the circulation, take it. A slightly delayed tube in a stable child beats an immediate tube in an arresting one.
✅ Checklist culture: why the boring card saves lives
Under stress your working memory collapses. You will forget something. The checklist is not bureaucracy. It is a cognitive offload. 🧠
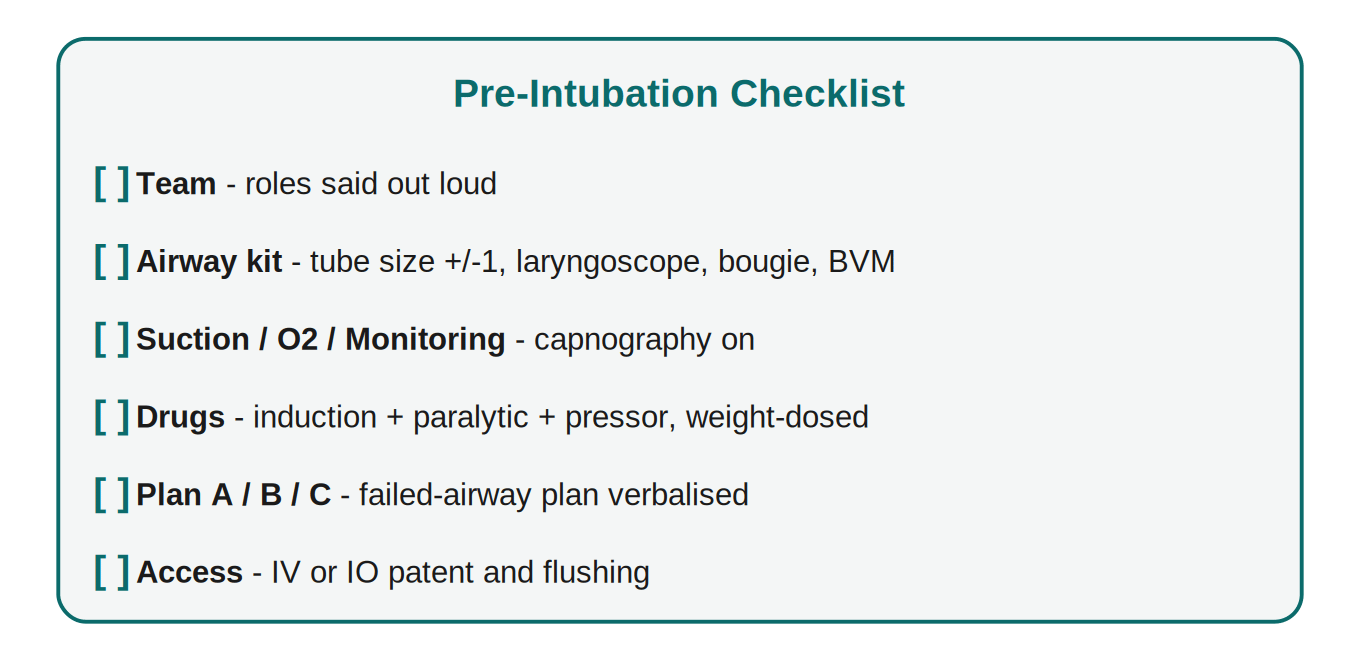
The pre-intubation checklist covers, at minimum:
🟩 Team: roles assigned. Who intubates, who pushes drugs, who does external laryngeal manipulation, who times and watches the sats.
🟩 Airway kit: correct tube size plus one above and one below, working laryngoscope (check the light), bougie or stylet, suction on and reachable, working bag-valve-mask.
🟩 Suction, oxygen, monitoring: waveform capnography attached and working before the attempt. No trace, no confirmation.
🟩 Drugs: induction and paralytic drawn, labelled, dosed to weight. Push-dose pressor ready if fragile.
🟩 Plan A, B, C: say the failed-airway plan out loud before you start. Everyone hears it.
🟩 Access: at least one reliable IV or IO, patent and flushing.
🗣️ A verbalised, shared checklist beats a silently ticked one. The point is shared situational awareness, not the paperwork.
🎯 The bottom line
The tube is the easy part. The optimisation is the medicine. 💊
Before you induce any sick child:
🫧 Oxygenate hard, then keep oxygen flowing through the apnoea.
🧍 Position for the age. Fix the geometry.
🩸 Resuscitate the circulation. Pressor and fluid ready, not hoped for.
✅ Run the checklist out loud, as a team.
Do these four and the peri-intubation arrest largely designs itself out.
Skip them and you are gambling with a child who has no reserve to spare.