
In the News: Hantavirus.
A slightly deep dive into why rats on a cruise is making the news.

🛳️ ICYMI 1 : Not just Sea Sickness
On April 1, 2026, the MV Hondius set sail from Ushuaia, Argentina, carrying 88 passengers and 59 crew on a polar expedition through Antarctica and the remote islands of the South Atlantic. It was supposed to be the trip of a lifetime.
Five days out, a 70-year-old male passenger developed fever, headache and mild diarrhoea. Then respiratory distress. Then he was dead by April 11. His body was removed when the ship docked at St. Helena. His wife, 69, became symptomatic days later and was evacuated to South Africa, where she too died.
By May 4, 2026, the WHO confirmed seven cases including three deaths. The ship, now stranded off the coast of Cape Verde with 150 people aboard, was refused permission to dock. Passengers were confined to cabins. Health officials in full PPE were photographed leaving the vessel. Three critically ill patients were airlifted to the Netherlands and Germany on May 5.
On May 6, 2026, the strain was confirmed: Andes virus, a hantavirus capable of rare human-to-human transmission through close contact.
147 people. Stranded at sea.
No cure.
No vaccine.
No specific treatment.
Can we all just catch a breath for a minute ?

The MV Hondius expedition cruise ship at sea
🎬 ICYMI 2: It Killed Gene Hackman’s Wife a Year Ago
In February 2025, Betsy Arakawa, the 65-year-old wife of Oscar-winning actor Gene Hackman, died from hantavirus pulmonary syndrome (HPS) at their home in Santa Fe. Hackman, 95 and living with advanced Alzheimer’s disease, died approximately one week later from cardiovascular disease. Their bodies and one of their three dogs were found together by maintenance workers two weeks after Arakawa’s death.
The investigation revealed Arakawa was last seen alive at a CVS pharmacy on February 11, 2025. She called a physician the next day but never made it to the appointment. She died at home from HPS. Rodent entry points were found on the property.
This case thrust hantavirus into the global spotlight.
And now, just over a year later, it is headlining international news again on the MV Hondius.
So what exactly is this virus?
And why should every emergency physician
and paediatrician know about it?
🦠 WHAT IS HANTAVIRUS?
Hantaviruses belong to the family Hantaviridae, genus Orthohantavirus. They are enveloped, single-stranded RNA viruses named after the Hantaan River in South Korea, where the first pathogenic strain was identified during the Korean War in the 1950s.
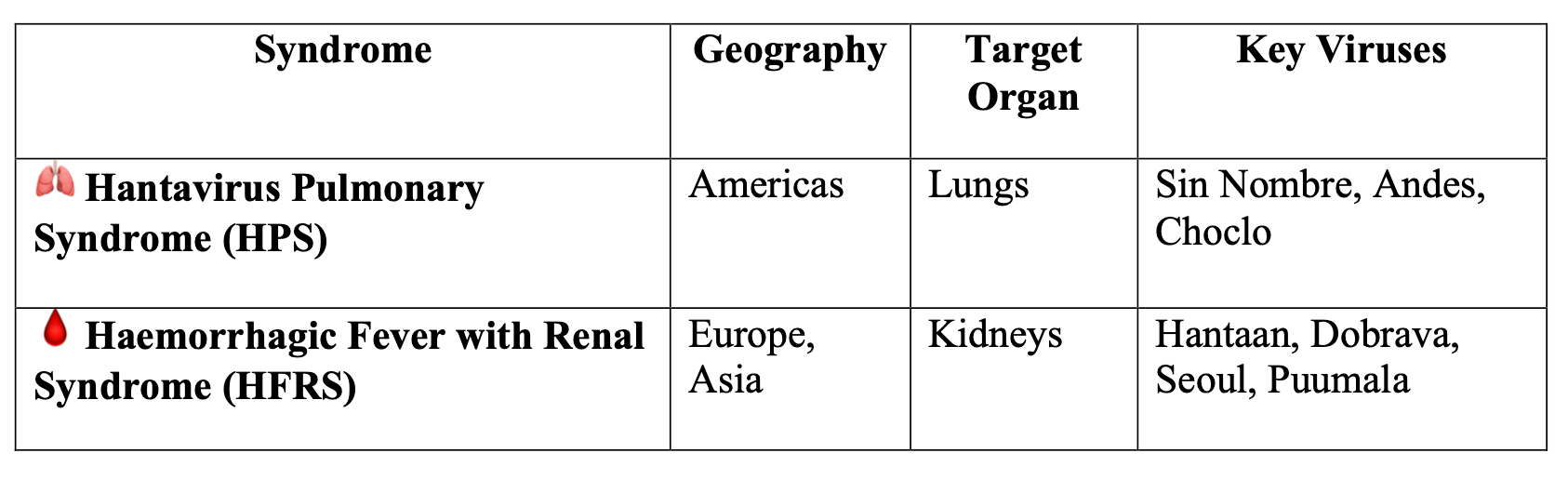
There are two major clinical syndromes:
A Recent Discovery
HPS was first described in 1993 during the infamous Four Corners outbreak in the American Southwest, when a cluster of previously healthy young Navajo people developed fatal respiratory failure.
The CDC identified a novel hantavirus (later named Sin Nombre virus, literally “the virus with no name”) carried by deer mice.

Transmission electron micrograph of Sin Nombre hantavirus]
🐀 HOW DO YOU CATCH IT?
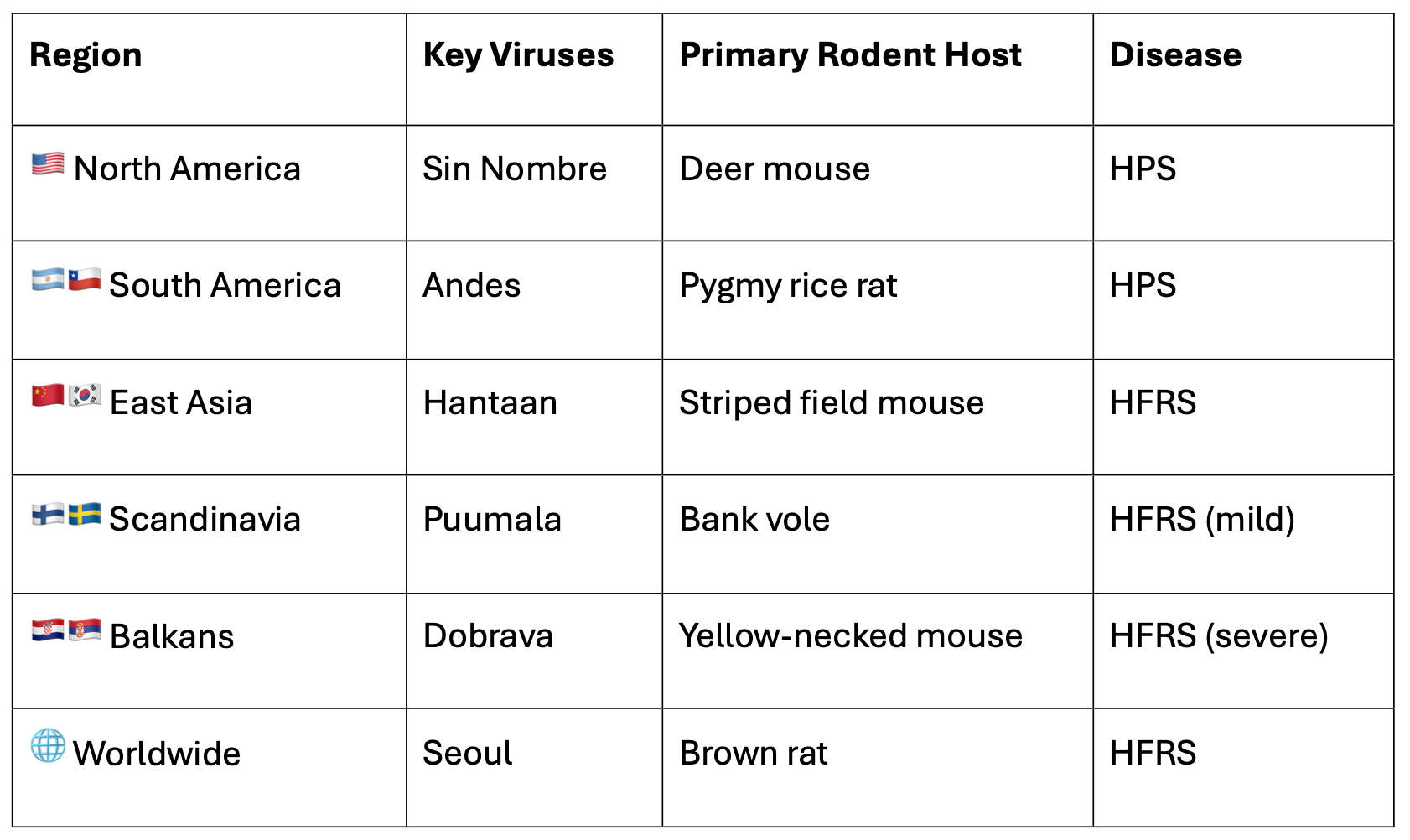
The natural reservoir is rodents. Different hantaviruses are carried by different rodent species:
🐭 Deer mouse (Peromyscus maniculatus) → Sin Nombre virus (North America)
🐭 Pygmy rice rat (Oligoryzomys longicaudatus) → Andes virus (South America)
🐭 Striped field mouse (Apodemus agrarius) → Hantaan virus (Asia)
🐭 Bank vole (Clethrionomys glareolus) → Puumala virus (Europe)

Routes of transmission:
🔸 Inhalation of aerosolised rodent urine, faeces or saliva (the BIG one)
🔸 Direct contact with rodent excreta through broken skin or mucous membranes
🔸 Rodent bites (rare)
🔸 Ingestion of contaminated food or water
⚠️ Critical point:
Sweeping or vacuuming rodent droppings aerosolises the virus. This is one of the most common exposure scenarios.
The CDC specifically warns: never dry-sweep rodent droppings.
Can it spread person-to-person?
For most hantaviruses: NO.
The major exception is Andes virus, the strain now confirmed on the MV Hondius. Andes virus has documented (though rare) person-to-person transmission through close contact. This is what makes the current cruise ship outbreak so alarming. The WHO confirmed on May 6, 2026 that human-to-human spread likely occurred among cabin-mates and spouses aboard the ship.
🏥 CLINICAL FEATURES: WHAT DOES HPS LOOK LIKE?
Yikes. This is where it gets ugly.
⏱️ Incubation Period
1 to 8 weeks after exposure (typically 2 to 4 weeks)
📋 Phase 1: Prodrome (3 to 5 days)
Looks like everything else in the ED. That is the problem.
🔹 Fever (often high, >38.5°C)
🔹 Myalgia (especially large muscle groups: thighs, hips, back)
🔹 Headache
🔹 Nausea, vomiting and diarrhoea
🔹 Malaise and fatigue
🔹 Dizziness
❌ What you WON’T see: Coryza, sore throat, rash.
This is NOT a typical upper respiratory infection.
📋 Phase 2: Cardiopulmonary Phase (rapid onset, 24 to 48 hours)
This is where patients crash. Hard. Fast.
🔴 Sudden onset of cough and dyspnoea
🔴 Non-cardiogenic pulmonary oedema (the lungs flood)
🔴 Bilateral infiltrates on CXR
🔴 Tachycardia progressing to arrhythmias
🔴 Hypotension progressing to cardiogenic shock
🔴 ARDS
The pathophysiology is vascular. Hantavirus infects pulmonary capillary endothelium, causing massive microvascular leak.
The lungs fill with fluid while the circulation loses volume. Patients drown from the inside while their blood pressure tanks.
Without adequate treatment, most deaths occur within 24 to 48 hours of entering the cardiopulmonary phase.
📋 Phase 3: Recovery (days to weeks)
Survivors typically become polyuric during convalescence and improve rapidly. But getting to this phase is the hard part.
🧪 LAB FINDINGS: THE DIAGNOSTIC CLUES
Here is where the smart clinician can catch this before the patient spirals.
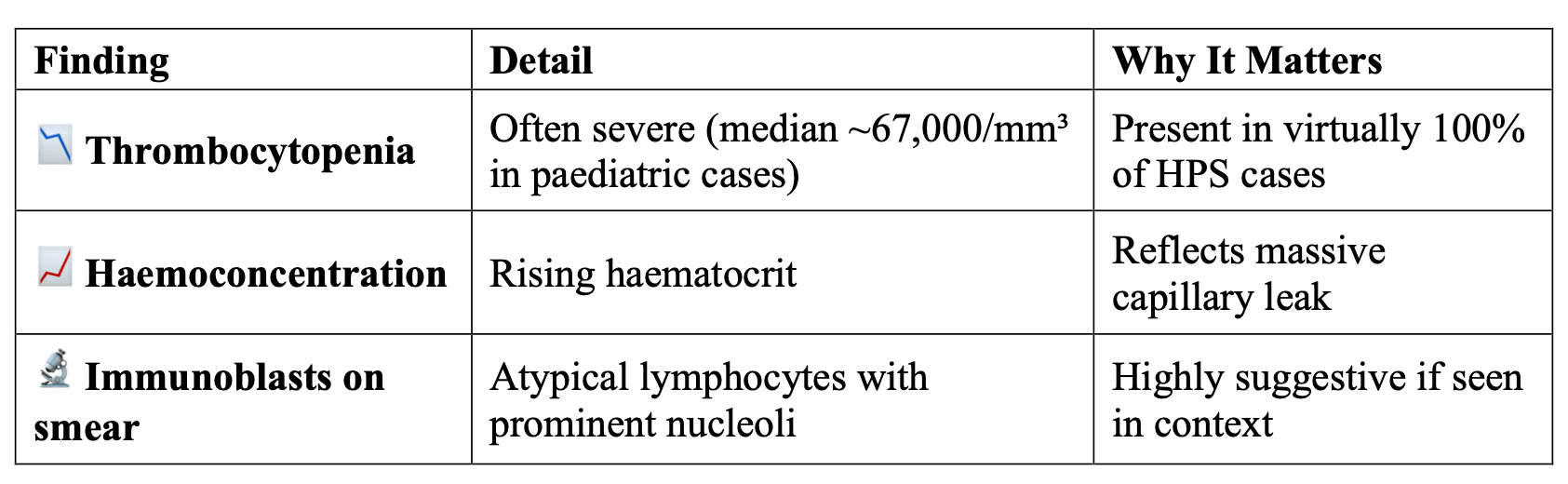
The classic HPS triad on bloods:
Other lab abnormalities:
🔸 Elevated LDH (often >1000 IU/L)
🔸 Elevated AST and ALT
🔸 Hypoalbuminaemia
🔸 Mildly elevated creatinine
🔸 Leukocytosis with left shift
🔸 Elevated PT (prothrombin time >14 seconds at admission was predictive of mortality in paediatric cases)
Definitive diagnosis:
🔬 Hantavirus-specific IgM (usually positive at symptom onset)
🔬 IgG antibodies (rise over time)
🔬 RT-PCR for hantavirus RNA
🔬 Immunohistochemistry on tissue
🔬 ELISA and immunofluorescent assays
⚡ ED pearl: If you see a febrile patient with thrombocytopenia, haemoconcentration and immunoblasts on the peripheral smear who is deteriorating rapidly with respiratory failure,
think hantavirus.
Especially with any history of rodent exposure or travel to endemic areas.
👶 HANTAVIRUS IN CHILDREN: WHAT PAEDIATRICIANS NEED TO KNOW
This is the bit most people miss. Hantavirus in kids is rare but man is it deadly.
The numbers:
From the largest US study (1993 to 2018, published in Pediatrics 2023):
🔹 Of 719 HPS patients, only 22 (3.0%) were aged 0 to 12 years and 47 (6.5%) were aged 13 to 18
🔹 Less than 10 to 15% of all cases are diagnosed in children
🔹 But the case fatality rate in children is 32 to 34%
🔹 Children with HPS die more quickly than adults
🔹 Elevated haematocrit and creatinine are specifically associated with death in children
Paediatric clinical features (from the Sin Nombre paediatric case series):
In 13 patients aged 10 to 16 years:
🔸 100% had fever, headache and cough/dyspnoea
🔸 90% had nausea or vomiting
🔸 80% had myalgia
🔸 67% had tachypnoea at admission
🔸 33% had hypotension at admission
🔸 92% developed full HPS
🔸 67% of HPS patients required mechanical ventilation
🔸 ECMO was used in 2 patients (1 survived)
Why is it underdiagnosed in children?
🤔 The prodrome looks like every other febrile illness in a child
🤔 Clinicians simply don’t think of it
🤔 Low overall incidence means low index of suspicion
🤔 Many cases likely occur at home in rural settings and are never tested
🤔 Family exposure clusters may be missed if only the adult is diagnosed
💊 TREATMENT: THERE ISN’T ONE (SORT OF)
Let’s be blunt:
there is no specific antiviral therapy for hantavirus.
Intravenous ribavirin was tested for HPS. It did not work.
Treatment is aggressive supportive care, ideally in an ICU:
The management approach:
🔹 Early recognition (this is the single biggest factor in survival)
🔹 Judicious fluid resuscitation (tricky because of capillary leak; overzealous fluids worsen pulmonary oedema)
🔹 Vasopressors for shock
🔹 Mechanical ventilation for respiratory failure
🔹 ECMO for refractory cardiopulmonary failure
🔹 Broad-spectrum antibiotics until diagnosis is confirmed (because the differential includes bacterial sepsis)
🔹 Avoid overhydration (the lungs are already leaking; more fluid = more oedema)
Early vasopressors are key.
📸 IMAGING
Chest X-ray findings in HPS:
🔸 Bilateral interstitial infiltrates progressing to alveolar infiltrates
🔸 Pulmonary oedema (non-cardiogenic pattern)
🔸 Pleural effusions (common)
🔸 Rapid progression over hours
🔸 Normal heart size (distinguishing it from cardiogenic pulmonary oedema)
The CXR can go from near-normal to complete whiteout in 24 hours.

🌍 GLOBAL DISTRIBUTION
Hantaviruses are found worldwide, but different strains dominate different regions:
Global distribution map of hantaviruses
What about Southeast Asia and Malaysia? 🇲🇾
Seoul virus (carried by brown rats, Rattus norvegicus) is present globally including in Southeast Asia.
While HPS is not typically reported in this region, HFRS cases and seroprevalence studies suggest that hantavirus circulation occurs.
The clinical relevance for Malaysian emergency physicians is primarily in the context of returning travellers from endemic HPS zones (the Americas) and recognition of Seoul virus-associated HFRS.
The differential includes:
🔸 Influenza / COVID-19 / RSV
🔸 Bacterial pneumonia / sepsis
🔸 Leptospirosis
🔸 Scrub typhus
🔸 Severe Dengue
🔸 Melioidosis (in our Southeast Asian context)
🔸 Plague (pneumonic)
📚 REFERENCES AND FURTHER READING
WHO Disease Outbreak News. Hantavirus cluster linked to cruise ship travel, Multi-country. 4 May 2026. https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON599
CDC. Clinician Brief: Hantavirus Pulmonary Syndrome (HPS). Updated March 2025. https://www.cdc.gov/hantavirus/hcp/clinical-overview/hps.html
Thorp L, Fullerton L, Whitesell A, Dehority W. Hantavirus Pulmonary Syndrome: 1993 to 2018. Pediatrics. 2023;151(4):e2022059352.
Ramos MM, Overturf GD, Crowley MR, et al. Infection with Sin Nombre hantavirus: clinical presentation and outcome in children and adolescents. Pediatrics. 2001;108(2):E27.
Pinto Junior VL, et al. Hantavirus pulmonary syndrome in children: case report and case series from an endemic area of Brazil. Rev Inst Med Trop Sao Paulo. 2019;61:e65.
Jonsson CB, Figueiredo LT, Vapalahti O. A global perspective on hantavirus ecology, epidemiology, and disease. Clin Microbiol Rev. 2010;23(2):412-441.
StatPearls. Hantavirus Pulmonary Syndrome. Updated April 2024. https://www.ncbi.nlm.nih.gov/books/NBK513243/
Duchin JS, et al. Hantavirus Pulmonary Syndrome: A Clinical Description of 17 Patients with a Newly Recognized Disease. NEJM. 1994;330(14):949-955.
Written for clinicians, trainees and anyone who wants to understand the news better.