
🧗 Don't Wait for the Cliff: When to Intubate in Paediatrics
Spoon Fed PEM | Paediatric Ventilation Series | Part 2

Intubation is not a treatment - it’s is a trade. You trade a failing or threatened airway and inadequate gas exchange for a controlled one and in return you accept the risks of laryngoscopy, positive pressure, sedation, haemodynamic collapse on induction and everything else that follows downstream in the PICU.
The decision is therefore never “can I intubate this child” but “does the benefit of taking the airway now exceed the cost of doing so, and the cost of waiting.”
Junior doctors get this wrong in two directions.
They intubate children who would have turned the corner on non-invasive support and they delay in children who were always going to need a tube, losing the controlled window and ending up doing it as a crash procedure in a peri-arrest state.
Both errors come from treating intubation as a numbers decision driven by a single blood gas or saturation reading. It is not. It is a trajectory decision.
🧭 This post gives you the frameworks to make that call.
🩺 The two questions (in oder)
Every intubation decision collapses into two sequential questions. Ask them in this order. Do not skip the first. 👆
🚨 Question 1: Is this child too sick to NOT intubate?
This is the override question. If the answer is yes, you stop deliberating and you secure the airway. There is no trial of non-invasive support, no further blood gas, no waiting for the registrar. These are the absolute indications, and they are mostly clinical, not biochemical.
🤔 Question 2: If not absolutely indicated, can we avoid it?
This is the harder, more common conversation. Most children in the resus bay are not in category one. They are working hard, they are tiring, their numbers are drifting, and you have a genuine choice. This is where trajectory, reversibility, and the failure of a non-invasive trial decide the outcome.
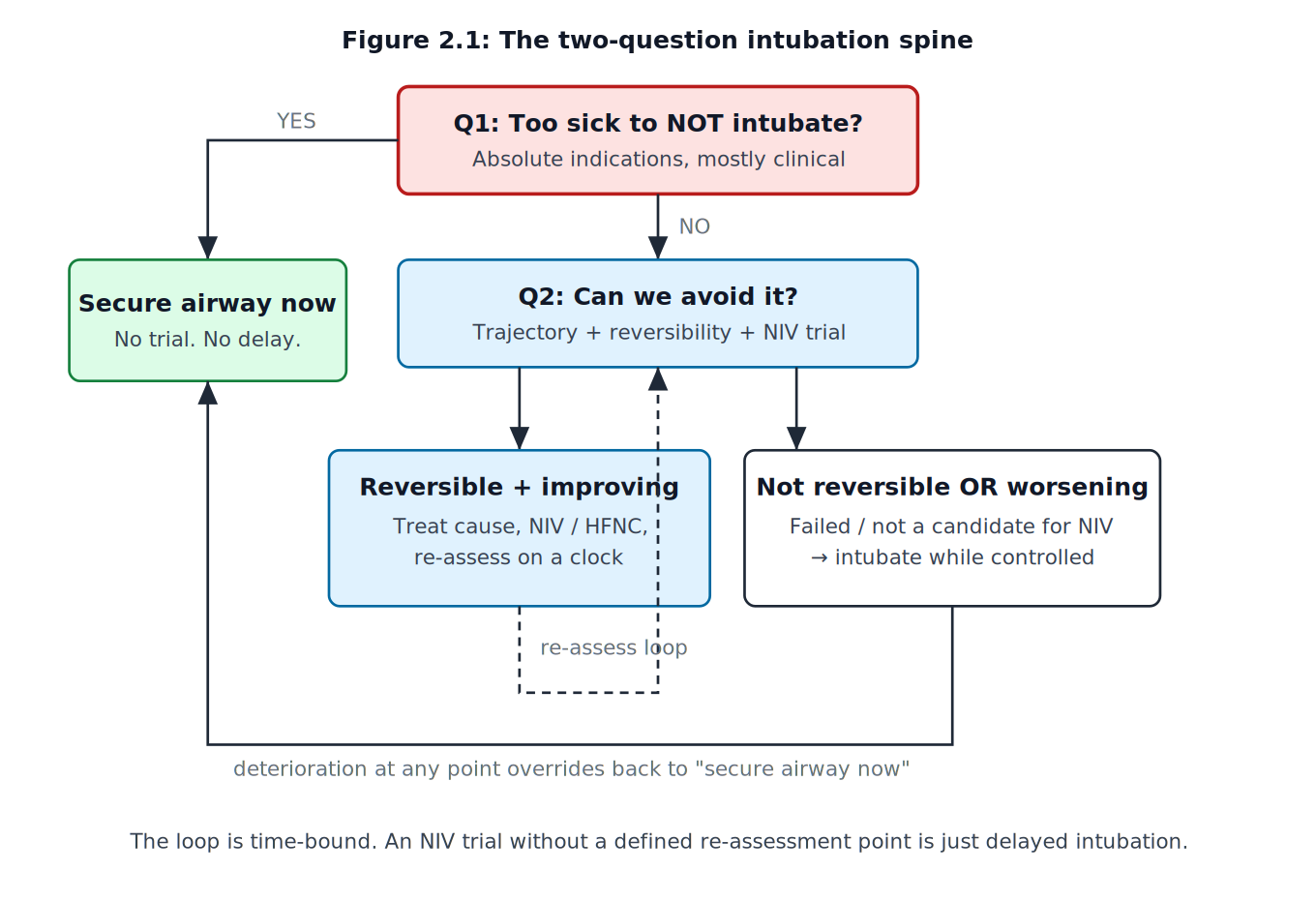
Figure 2.1: The two-question intubation spine
🚨 Question 1: The absolute indications
These are the situations where deliberation itself is the error. Commit them to memory as clinical patterns, not numbers.
🔥 Failure or imminent loss of airway patency.
A child who cannot protect or maintain their own airway needs it secured regardless of gas exchange.
This includes deepening obstruction such as : expanding neck haematoma, progressive angioedema, severe epiglottitis or croup unresponsive to treatment, airway burns with rising stridor, and the obtunded child whose tongue and secretions are the obstruction.
The relevant question is whether the airway will still be patent in ten minutes, not whether it is patent now. A partially obstructed airway that you can still intubate is a far better proposition than a completely obstructed one that you cannot.
💤 Apnoea or inadequate respiratory drive.
Central depression from raised intracranial pressure, status epilepticus, poisoning or primary CNS pathology.
If the child is not breathing adequately and the cause is not instantly reversible (opioid reversal, glucose, a brief postictal pause that resolves), you ventilate.
🫁 Failure of oxygenation or ventilation despite maximal non-invasive support. This is not a single low saturation.
It is persistent, refractory hypoxaemia or hypercapnic acidosis that has not responded to escalating non-invasive measures.
The trajectory and the response to treatment matter more than the absolute value.
🧠 The need to control physiology that cannot be controlled awake.
Severe traumatic brain injury requiring tight CO2 control, the child requiring deep sedation for an emergent procedure or imaging in an unstable state, status epilepticus requiring agents that abolish respiratory drive or significant burns requiring transfer where the airway will predictably deteriorate en route.
Here you intubate not because the airway has failed but because you are choosing to take control of it pre-emptively.
⏩ Anticipated clinical course.
This is the most under-weighted indication and the one juniors miss most. A child who is currently compensating but whose underlying disease will predictably worsen, especially before or during transfer, should be intubated in the controlled environment of the resus bay rather than in the back of a retrieval ambulance.
“They are stable now” is not reassurance if the trajectory is downward and the next safe window to act is hours away.
🤔 Question 2: Can we avoid it?
Most of your decisions live here. The child is working hard, the numbers are not catastrophic, and you have a real choice. Three things decide it: reversibility, trajectory, and the response to a time-bound trial.
🔁 Reversibility
Is the underlying problem something you can fix faster than the child will tire? Bronchospasm responds to bronchodilators and steroids over minutes to hours. Pulmonary oedema responds to diuresis and pressure offloading.
A supraventricular tachycardia driving respiratory distress responds to adenosine in seconds. If the cause is reversible on a timescale shorter than the child’s respiratory reserve, you have grounds to support rather than intubate.
The inverse is the trap.
A fixed or progressive disease process (a large effusion, worsening ARDS, an evolving neurological catastrophe) will not be talked out of failing by CPAP. Non-invasive support here only delays the inevitable and burns the controlled window.
📈 Trajectory beats snapshot
A single observation tells you almost nothing. Two observations separated by time tell you almost everything.
The child whose work of breathing, gas exchange, and conscious level are stable or improving over thirty to sixty minutes of treatment is winning. The child going the other way is losing, and the rate of change predicts how much time you have.
This is why you document serial observations, not isolated ones.
A pH of 7.28 that was 7.34 an hour ago is a different child from a pH of 7.28 that was 7.22 an hour ago.
The number is identical.
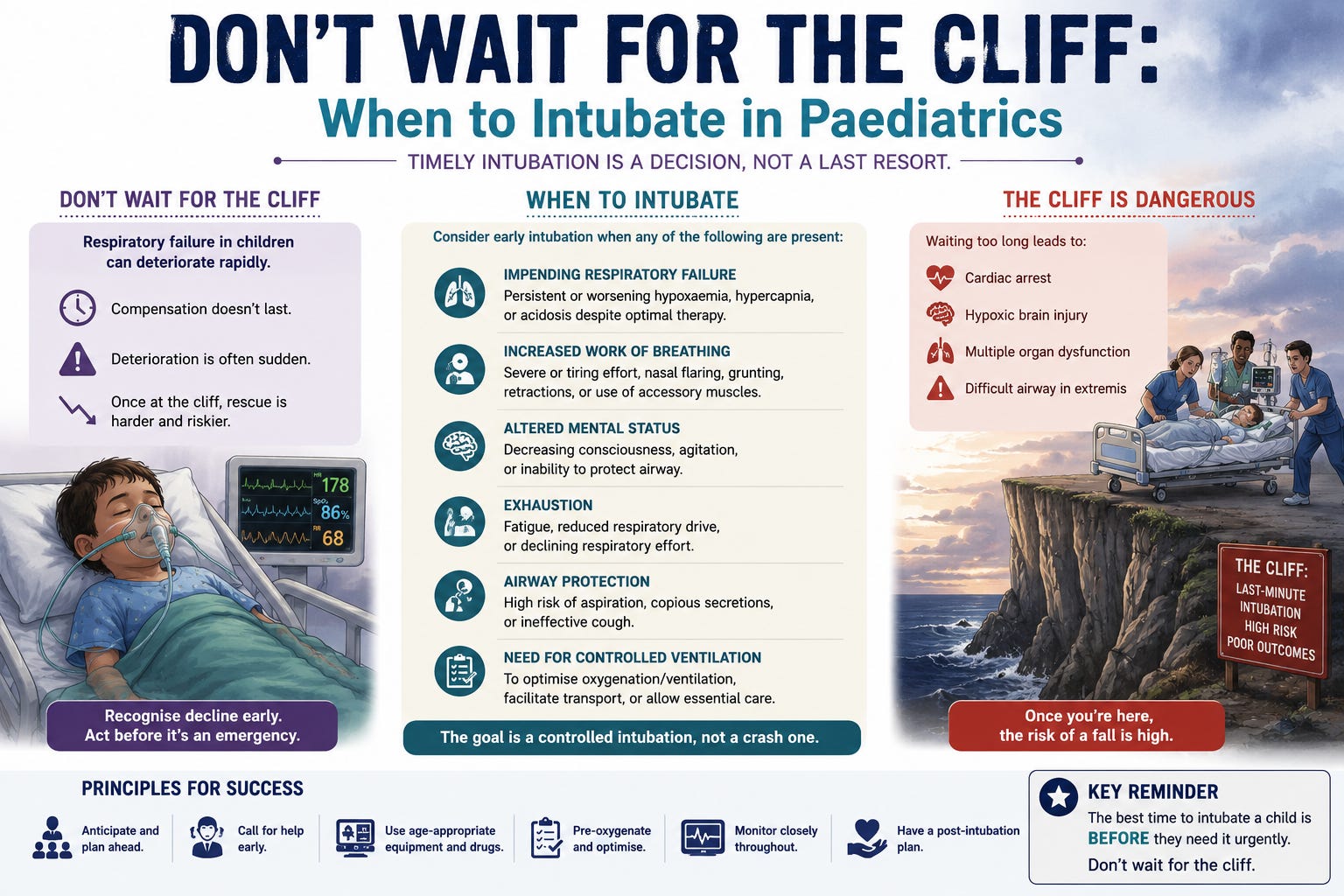
🧗 Paediatric reserve and the cliff
Children compensate well and then fail fast.
This is a recurring theme of this series, established physiologically in Part 1: high oxygen consumption, low functional residual capacity relative to closing capacity, and a chest wall that contributes little mechanical advantage.
The practical consequence for this decision is brutal.
The clinical signs of compensation (tachypnoea, recruitment of accessory muscles, tachycardia) can look stable right up until they are not, and the transition from “working hard but holding” to “arrested” is shorter than in an adult.
The dangerous signs are the ones that indicate compensation is ending: a falling respiratory rate in a child who has been tachypnoeic and is now tiring, a rising then falling conscious level, bradycardia, and silent chest.
By the time these appear you have left the controlled window.
🚩 Do not wait for them to appear.
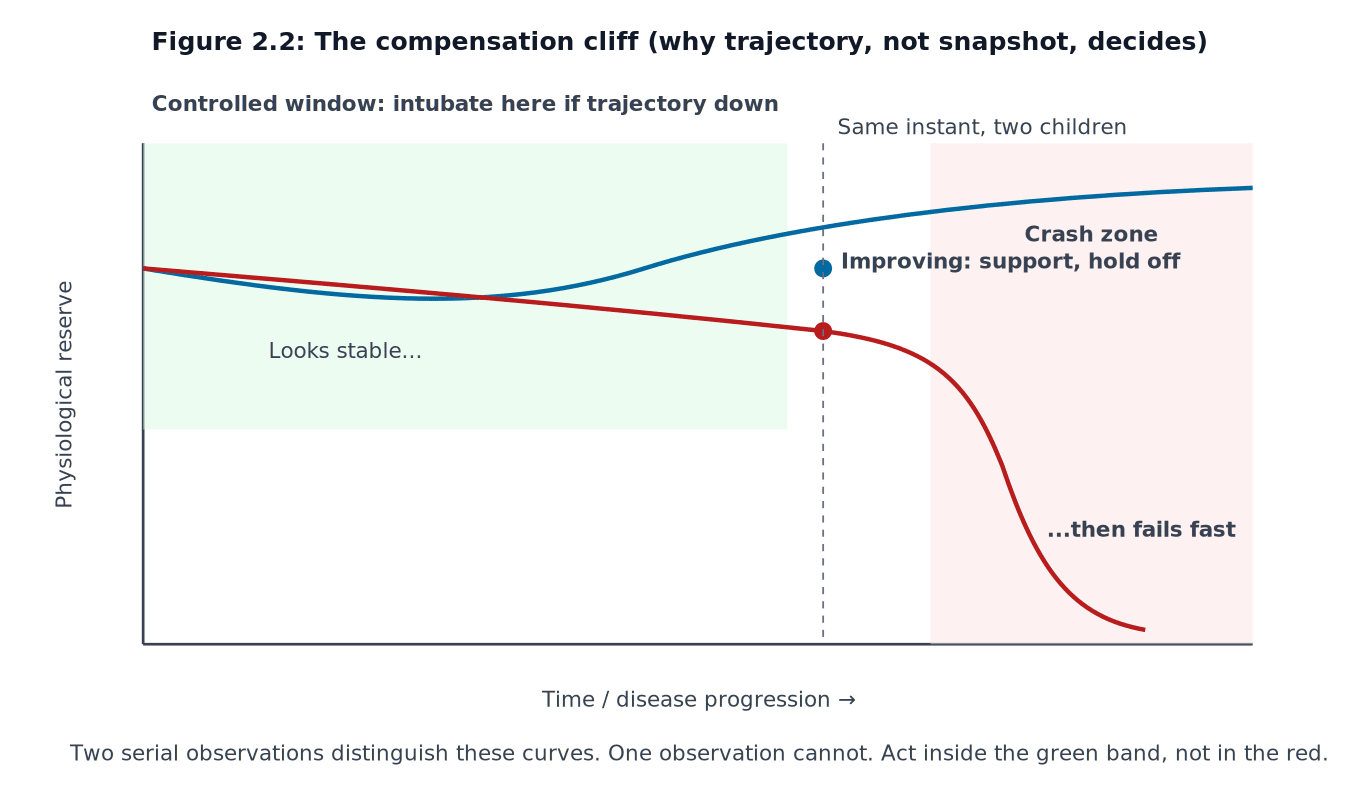
Figure 2.2: The compensation cliff (why trajectory, not snapshot - decides what happens next)
⏱️ The time-bound trial
If you elect to support rather than intubate, you are running a trial. A trial without a stop rule is not a clinical plan, it is hope. Before you start non-invasive support, define three things out loud and write them down:
🎯 What you expect to improve. Work of breathing, gas exchange, conscious level. Be specific.
⏰ By when. A defined re-assessment point. Minutes, not “later.” For most acute respiratory failure this is a short interval, on the order of an hour or less, with continuous observation in between.
🛑 What failure looks like. The threshold that converts the trial into an intubation. Worsening on any of your chosen parameters, no improvement by the re-assessment point, rising sedation requirement to tolerate the interface, or a falling conscious level.
The failure of a non-invasive trial is itself a recognised indication for intubation. The point of declaring the stop rule in advance is that it removes the sunk-cost reasoning that keeps tired teams persisting with a failing trial because they have already invested in it.
Sunk cost reasoning (often known as the sunk cost fallacy) is the psychological tendency to continue a failing endeavour - such as a project, relationship or investment simply because you have already invested time, money, or effort into it.
The child does not care how much CPAP you have already given.
💯 They care whether it is working.
A note on non-invasive support as a bridge versus a destination: it is reasonable as a bridge while a reversible cause is treated, and it is reasonable as a ceiling of care decided in advance.
It is dangerous when it drifts into being neither, used to avoid a decision rather than to enact one.
⚠️ The crash-intubation trap
💀 The worst intubation is the one you are forced into.
When you wait past the controlled window, you intubate a child who is hypoxic, acidotic, haemodynamically marginal and physiologically intolerant of the apnoea and the induction agents.
Every part of the procedure is harder and every complication is more likely.
Desaturation is faster because the reserve is already gone.
Induction agents drop a blood pressure that was already being propped up by endogenous catecholamines.
The first attempt matters more because there is no buffer for a second.
Junior doctors instinctively frame early intubation as escalation and waiting as conservatism.
In a child who is going to need it, that framing is inverted.
Waiting is the high-risk choice.
⚠️ Acting early while you still have reserve, help, and a controlled environment is the conservative one.
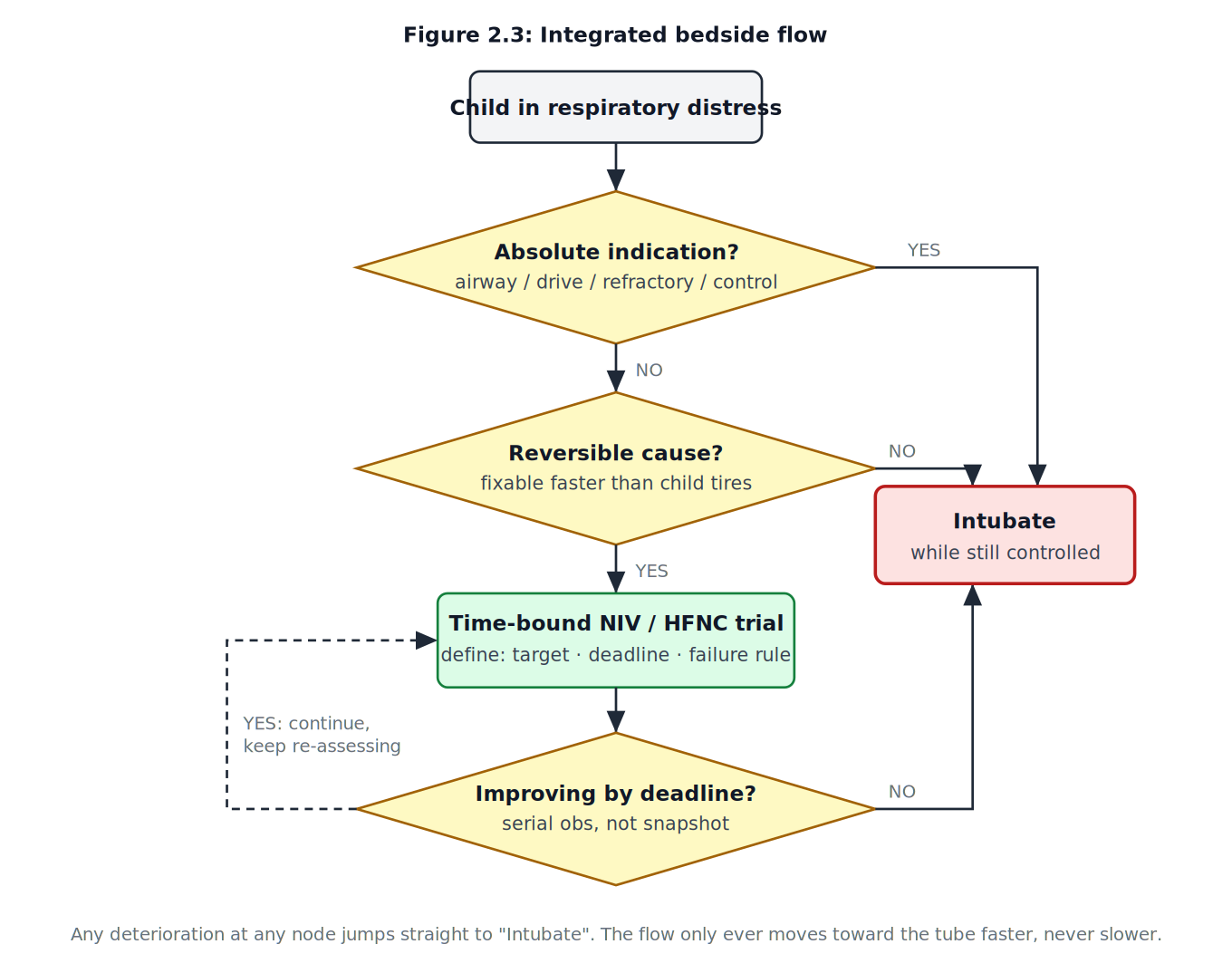
Figure 2.3: Integrated bedside flow
🩺 What this looks like at the bedside
🚨 Override check first. Failing airway, absent drive, refractory to max support, or physiology you can’t control awake? → secure the airway now, stop reading gases.
🤔 Then the avoidability check. Not reversible faster than the child will tire? → intubate now while it’s controlled. Reversible? → run a time-bound trial with a target, deadline, and stated failure rule, and watch the trajectory, not a single number.
🧗 The paediatric truth underneath it all: the child looks like they’re coping until just before they aren’t. Decompensation signs arrive late, the cliff is steep, and the controlled window closes quietly. ⏳
🔑 The one reframe to keep: in a child who’s going to need a tube, early intubation is the conservative choice and waiting is the gamble. Harm comes from being forced to act too late, not from acting too early.
🔜 Coming next
Part 3 takes the decision you have just made and turns it into a safe procedure: rapid sequence induction in children.
Drug selection and weight-based dosing, the physiologically difficult paediatric airway, apnoeic oxygenation and pre-oxygenation that actually buys you time, and how induction agents behave in the shocked child.
The decision to intubate is only as good as the first attempt that follows it. 🎯
This series is educational and written for junior doctors building a structured understanding of paediatric ventilation. It does not replace local PICU, anaesthetic, and retrieval-service protocols, senior clinical judgement, or formal airway training.